Question: What 3 historical factors can help establish that a transient loss of vision reported to be unilateral by the patient is consistent with the visual aura of migraine?
 1
1
Question: What 3 historical factors can help establish that a transient loss of vision reported to be unilateral by the patient is consistent with the visual aura of migraine?
1
Questions: Transient monocular vision loss with:
1. Headache, scalp tenderness, jaw claudication, and diplopia suggest?
2. Eye or brow pain suggests?
3. Neck pain suggests?
4. Ipsilateral Horner syndrome suggests?
5. Simultaneous contralateral hemisensory or motor findings suggests?
6. Presyncope suggests?
7. When moving the eye suggests?
8. Blurry vision when reading suggests?
Question: Which of the following are correct?
1. If visual acuity can be improved by the patient looking through a pinhole, the problem is refractive or ocular, not neurologic in origin.
2. Reduction in the saturation or brightness of colors may be an early sign of optic nerve disease.
3. A relative afferent pupillary defect ipsilateral to visual loss indicates an optic neuropathy or severe retinal disease (in which case the retina looks abnormal on funduscopic examination).
4. If nonorganic visual loss is suspected, normal stereovision indicates 20/20 visual acuity in both eyes.
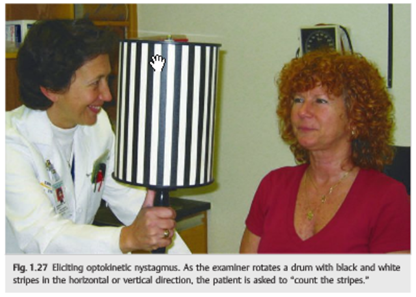
5. A positive response to the optokinetic nystagmus stimulus indicates a visual acuity of at least 20/400 in the eye tested.
Question: Which of the following are correct?
1. Fat is hyperintense on T1.
2. Vitreous is hyperintense on T1.
3. CSF is hyperintense on T1.
4. Subacute blood is hyperintense on T1.
5. Fat is hypointense on T2.
6. Vitreous is hypointense on T2.
7. CSF is hypointense on T2.
8. Diffusion-weighted images are ideal in detecting acute cerebral ischemia.
9. T2 gradient echo allows better visualization of blood products, such as hemosiderin.
Question: On CT which of the following are isodense, hypodense, hyperdense, or enhance on contrast?
1 Acute clot in a large vessel
2 Blood vessels
3 Bone
4 Breakdown of the normal blood-brain barrier
5 Calcium
6 Edema
7 Fat
8 Fresh blood
9 Infarction
10 Inflammatory lesions
11 Necrosis
12 Neoplasms
13 Normal brain

Question: Which of the following are good indications for CT and which for MRI?
1 Bone lesions
2 Brain lesions
3 Chiasmal syndrome
4 Fungal sinusitis
5 Infectious or noninfectious orbital inflammation
6 Lacrimal gland lesions
7 Lesions that may contain calcium
8 Ocular trauma to rule out a foreign body
9 Optic neuropathy
10 Orbital apex or cavernous sinus syndrome
11 Orbital trauma
12 Preoperative imaging for orbital disease when imaging of the facial sinuses is very important
13 Suspected optic nerve tumor
14 Wooden foreign body
Question: What are 7 indications for B-scan echography?
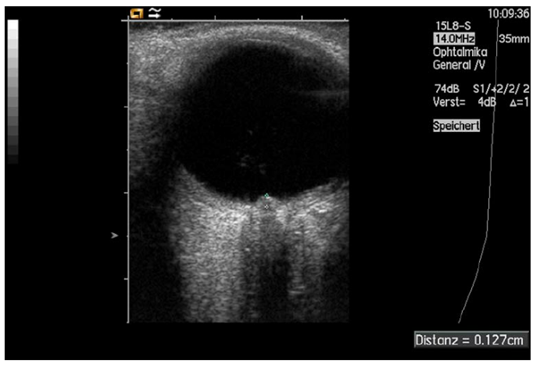
Fig. 8. Measurement of papilledema using ultrasound: disc elevation is quantified by putting the first caliper on the uppermost part of the swollen disc; the second caliper is positioned on the strongly reflecting line representing the lamina cribrosa 8
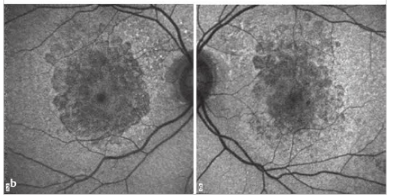
Question: Which of the following are hyperautofluorescent?
1. Optic Disc Drusen
2. Papilledema
3. Accumulation of lipofuscin in the retinal pigment epithelium
4. Loss of lipofuscin in the retinal pigment epithelium
5. Central serous chorioretinopathy
6. Best disease
 1
1
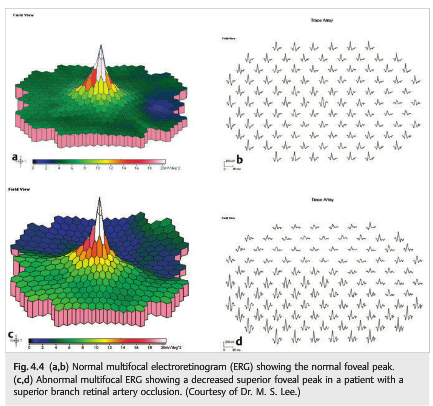
Which of the following statements are correct?
1. Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss.
2. The ERG is invariably severely depressed by the time patients complain of visual loss.
3. In full-field ERG the responses cannot be substantially altered voluntarily.
4. The full-field ERG may be normal in minor or localized retinal disease, particularly maculopathies, even with severe visual acuity loss.
5. Multifocal ERG is extremely helpful in detecting occult focal retinal abnormalities within the macula.
6. Uncooperative patients can alter the responses on a multifocal ERG by not fixating accurately.
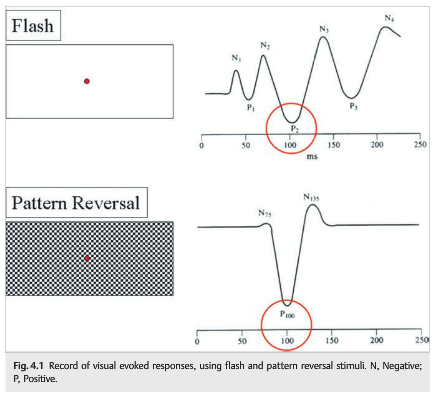
Question: Which of the following are correct for visual evoked responses?
1.Abnormal responses may occur if the patient does not look at the screen, does not focus on the screen, moves the tested eye, or is tired.
2. Appropriate refraction is necessary.
3. The visual evoked response reflects the integrity of the afferent visual pathway (damage anywhere from the retina to the occipital cortex may alter the signal).
4. It is primarily a function of central visual function because such a large region of the occipital cortex near the recording electrodes is devoted to macular projections.
5. Visual evoked responses are not useful in evaluating the integrity of the visual pathway in infants and inarticulate adults.
6. Visual evoked responses cannot provide an estimate of visual acuity when stimuli of various sizes are used.
 1
1