Recommended Reading – Terson Syndrome
Terson syndrome in subarachnoid hemorrhage, intracerebral hemorrhage, and traumatic brain injury. Czorlich P, Skevas C, Knospe V, Vettorazzi E, Richard G, Wagenfeld L, Westphal M. Regelsberger J. Neurosurgical Review. 2015,38,1,129–136
Abstract
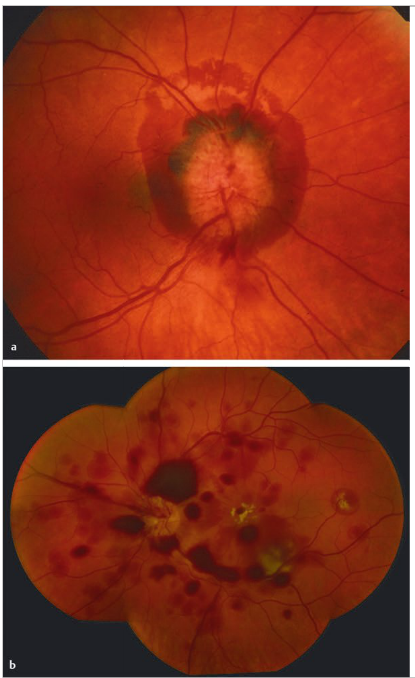
This prospective trial was designed to evaluate the incidence of Terson syndrome in patients suffering from subarachnoid hemorrhage, intracerebral hemorrhage, or traumatic brain injury and whether consequences necessarily derive from the intraocular hemorrhage itself. Two ophthalmologic examinations were performed to identify patients with Terson syndrome. Data on initial Glasgow Coma Scale, Hunt and Hess and Fisher grades, aneurysm site and diameter, and volume of hemorrhage in intracerebral hemorrhage patients were correlated to the location and course of Terson syndrome. Follow-up was performed after 3 months, including clinical and ophthalmologic investigations. The data showed that 16 of 83 subarachnoid hemorrhage patients (19.3 %), 2 of 22 intracerebral hemorrhage patients (9.1 %), and 1 of 32 traumatic brain injury patients (3.1 %) suffered from Terson syndrome. Low Glasgow Coma Scale (p = 0.002), high Hunt and Hess grade (p < 0.001), and high Fisher grade (p = 0.002) were found to be associated with a higher incidence of Terson syndrome. The neurological outcome in subarachnoid hemorrhage patients suffering from Terson syndrome was worse compared with that of subarachnoid hemorrhage patients without Terson syndrome (p = 0.005), and vitrectomy was performed in seven eyes of six patients due to poor visual acuity. Terson syndrome is underestimated in patients with subarachnoid hemorrhage and a rare pathology in intracerebral hemorrhage as well as in traumatic brain injury patients. Spontaneous regression of the intraocular hemorrhage may be seen, but in half of the patients, vitrectomy is necessary to prevent permanent visual deterioration.
Full-Text PDF https://drive.google.com/open?id=1UYiSRw8j3r5qgjAcmVDJtmyW264WWE-y