Which of the following statements are correct?
1. Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss.
2. The ERG is invariably severely depressed by the time patients complain of visual loss.
3. In full-field ERG the responses cannot be substantially altered voluntarily.
4. The full-field ERG may be normal in minor or localized retinal disease, particularly maculopathies, even with severe visual acuity loss.
5. Multifocal ERG is extremely helpful in detecting occult focal retinal abnormalities within the macula.
6. Uncooperative patients can alter the responses on a multifocal ERG by not fixating accurately.
____________________________________________________
Answers: All are correct.
Explanation:
“Electroretinogram
The electroretinogram (ERG) is a measurement of electrical activity of the retina in response to light stimulus. It is measured at the corneal surface by electrodes embedded in a corneal contact lens worn for testing. The ERG is normal in optic neuropathies.
Full-Field Electroretinogram
A full-field ERG is generated by stimulating the entire retina with a flash light source under varying conditions of retinal adaptation to dark and light (▶Fig. 4.3).
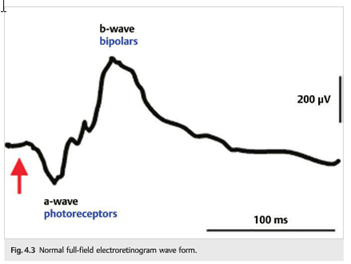
Major components of the electrical waveform generated and measured include the following:
- A wave (negative): primarily derived from the photoreceptor layer (outer retina)
- B wave (positive): derived from the inner retina (Müller and bipolar cells)
- Two other waveforms that are sometimes recorded are the c-wave originating in the pigment epithelium and the d-wave indicating activity of the OFF bipolar cells.
Rod and cone photoreceptors can be separated by varying stimuli and the state of retinal adaptation during testing.
Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss. Disorders such as retinitis pigmentosa, cone–rod dystrophy, toxic retinopathies, and retinal paraneoplastic syndromes may present with variably severe visual loss and minimally visible retinal abnormalities. The ERG is invariably severely depressed by the time patients complain of visual loss, making full-field ERG testing very useful. Although poorly cooperative patients can make interpretation of the full-field ERG more difficult (there can be background noise due to frequent blinking and squeezing), the responses cannot be substantially altered voluntarily (unlike visual evoked responses).
Because the full-field ERG measures only a mass response of the entire retina, it may be normal in minor or localized retinal disease, particularly maculopathies, even with severe visual acuity loss.
Multifocal Electroretinogram
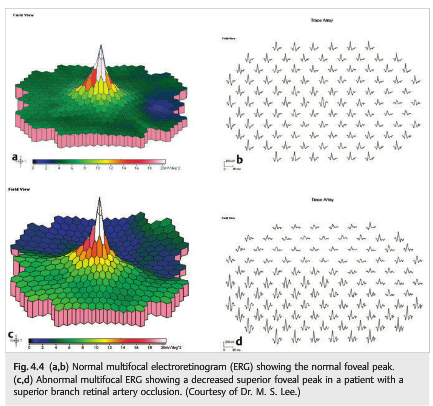
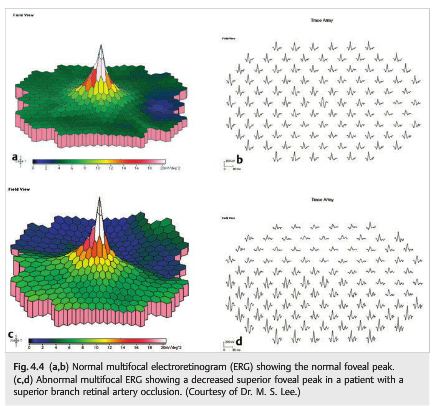
Multifocal ERG simultaneously records ERG signals from up to 250 focal retinal locations within the central 30 degrees. The individual responses are mapped topographically (▶Fig. 4.4).
This technique is extremely helpful in detecting occult focal retinal abnormalities within the macula. Unlike full-field ERG, however, uncooperative patients can alter the responses on a multifocal ERG by not fixating accurately.
 ”1
”1
Because electrophysiologic testing often provides diagnostic clues as to the etiology of the unexplained visual loss, it should be part of the neuro-ophthalmologic examination in selected patients.2
References:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
2. Electrophysiologic Tests. 2005 Hoyt & Walsh. Spencer S. Eccles Health Sciences Library. North American Neuro-Ophthalmology Association (NANOS), 2012. https://collections.lib.utah.edu/details?id=186706&q=erg&page=1&rows=25&fd=title_t%2Csetname_s%2Ctype_t&sort=&gallery=#t_186706
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.