Recommended Reading – Ocular myasthenia gravis: an update on diagnosis and treatment
Ocular myasthenia gravis: an update on diagnosis and treatment
Elizabeth Fortina, Dean M. Cestaria, and David H. Weinberg
Current Opinion in Ophthalmology. 2018.29:6
Purpose of review
Myasthenia gravis is an autoimmune disease that commonly affects the palpebral and extraocular muscles. Ocular myasthenia gravis (OMG) is a variant of the disease that is confined to the ocular muscles but frequently becomes generalized over time. The diagnosis of OMG is often challenging but both clinical and laboratory findings are helpful in confirming the clinical suspicion. This review provides an update on the diagnostic approach and therapeutic options for OMG.
Recent findings
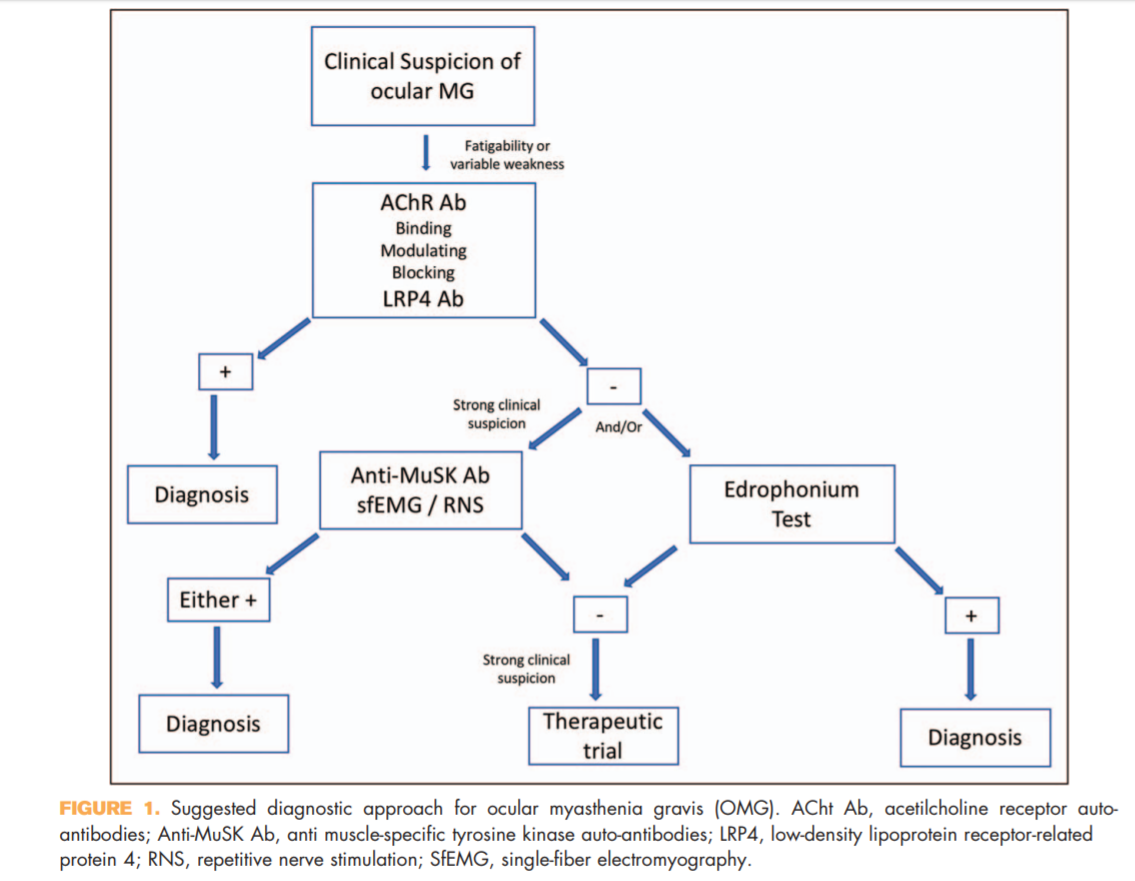
Antimuscle-specific tyrosine kinase and LDL-related receptor-related protein 4 are newly available serologictesting for myasthenia gravis that can help in increasing the diagnostic sensitivity of OMG. They should be included to the diagnostic algorithm of OMG in appropriate clinical situations.
Summary
OMG remains a primarily clinical diagnosis, but recent advances in laboratory testing can improve the diagnostic accuracy and should be used in appropriate clinical settings. The mainstay of treatment for OMG has not significantly changed over the past years, but the increasing availability of steroid-sparing agents improved the disease control while minimizing steroid-induced complications.
KEY POINTS
● OMG remains a clinical diagnosis, but various laboratory and electrophysiologic testing can help in increasing the diagnostic accuracy.
● Antimuscle-specific tyrosine kinase and LDL-related receptor-related protein 4 antibodies should be included in the diagnostic algorithm of patients suspected to have OMG.
● Therapy should aim at achieving satisfactory symptomatic control while reducing minimizing
Full Text https://drive.google.com/open?id=1ArU1gdYCwKWogLDCr0OcslzGd6egLN8y