Questions:
7. What differentiates classic from symptomatic trigeminal neuralgia?
8. Name several triggers for trigeminal neuralgia?
9. For Classic Trigeminal Neuralgia, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment
10. For Symptomatic Trigeminal Neuralgia, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment
11. For Cluster (Histamine) Headache, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment
12. For Episodic or Chronic Paroxysmal Hemicrania, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment
13. For SUNCT Syndrome (Short-lasting, Unilateral, Neuralgiform headache attacks with Conjunctival injection and Tearing), what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment
14. For Hemicrania Continua, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment
____________________________________________________
Questions with answers:
7. What differentiates classic from symptomatic trigeminal neuralgia?
The classic form is to be considered idiopathic. It includes the cases that are due to a normal artery in contact with the 5th nerve, such as the superior cerebellar artery or even a primitive trigeminal artery. The symptomatic form is not idiopathic and can have multiple origins: aneurysms, tumors, chronic meningeal inflammation, or other lesions may irritate trigeminal nerve roots along the pons. An abnormal vascular course of the superior cerebellar artery is often cited as the cause.
8. Name several triggers for trigeminal neuralgia?
1. Chewing, talking or smiling
2. Drinking cold or hot liquids
3. Touching, shaving, teeth brushing, nose-blowing
4. Drafts of cold air
9. For Classic Trigeminal Neuralgia, what are the:
1. Age range: 50-year-old
2. Gender ratio: 1/4
3. Location of pain: Unilateral V2 & V3 > V1
4. Type of pain: Stabbing
5. Duration of pain: <1 second
6. Temporal pain profile: Few to many/day for weeks to months. Pain-free between attacks.
7. Associated signs: No associated signs, look for triggers
8. Interictal exam: Normal
9. Treatment: Carbamazepine (Tegretol) frequent good response
10. For Symptomatic Trigeminal Neuralgia, what are the:
1. Age range: Any
2. Gender ratio: M=F
3. Location of pain: May be bilateral, V1, 2 or 3
4. Type of pain: Dull, persistent
5. Duration of pain: Chronic
6. Temporal pain profile: Fluctuations but no remission
7. Associated signs: 5th nerve hypoesthesia, dysesthesia, and motor deficit
and other cranial nerve palsies
8. Interictal exam: 5th nerve hypoesthesia and motor deficit
9. Treatment: Variable response to therapy
11. For Cluster (Histamine) Headache, what are the:
1. Age range: Young
2. Gender ratio: M/F 9/1
3. Location of pain: Unilateral periorbital
4. Type of pain: Boring, very severe
5. Duration of pain: 15-180 minutes
6. Temporal pain profile: 1-8/day, attack phase 4-16 weeks, Remission 6-24 months
7. Associated signs: Horner syndrome, eye redness, tearing and rhinorrhea
8. Interictal exam: Normal but may have Horner syndrome
9. Treatment: Acute: oxygen, injectable triptans, and DHE, Chronic: lithium, steroids, channel inhibitors-Verapamil (Calan)
12. For Episodic or Chronic Paroxysmal Hemicrania, what are the:
1. Age range: any
2. Gender ratio: M/F 1/3
3. Location of pain: Unilateral periorbital
4. Type of pain: Very severe
5. Duration of pain: 2-30 minutes
6. Temporal pain profile: 5/day
7. Associated signs: Horner syndrome, eye redness, tearing and rhinorrhea
8. Interictal exam: Normal but may have Horner syndrome
9. Treatment: Indomethacin stops pain
13. For SUNCT Syndrome (Short-lasting, Unilateral, Neuralgiform headache attacks with Conjunctival injection and Tearing), what are the:
1. Age range: Any
2. Gender ratio: M/F 8/1
3. Location of pain: Unilateral periorbital
4. Type of pain: Very severe
5. Duration of pain: 5-240 seconds
6. Temporal pain profile: Numerous in a day, sometimes dull pain between attacks, remissions with an irregular pattern
7. Associated signs: Eye redness and tearing
8. Interictal exam: Normal
9. Treatment: None, variable response (Corticosteroids and the antiepileptic drugs gabapentin, lamotrigine, and carbamazepine may help relieve some symptoms)
14. For Hemicrania Continua, what are the:
1. Age range: Any
2. Gender ratio: M>F
3. Location of pain: Unilateral hemicrania, always same side
4. Type of pain: Sharp pain
5. Duration of pain: <1 minute
6. Temporal pain profile: Associated with a continuous headache of fluctuating intensity
7. Associated signs: Nausea, vomiting, photophobia and may have Horner syndrome
8. Interictal exam: Normal
9. Treatment: Indomethacin
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
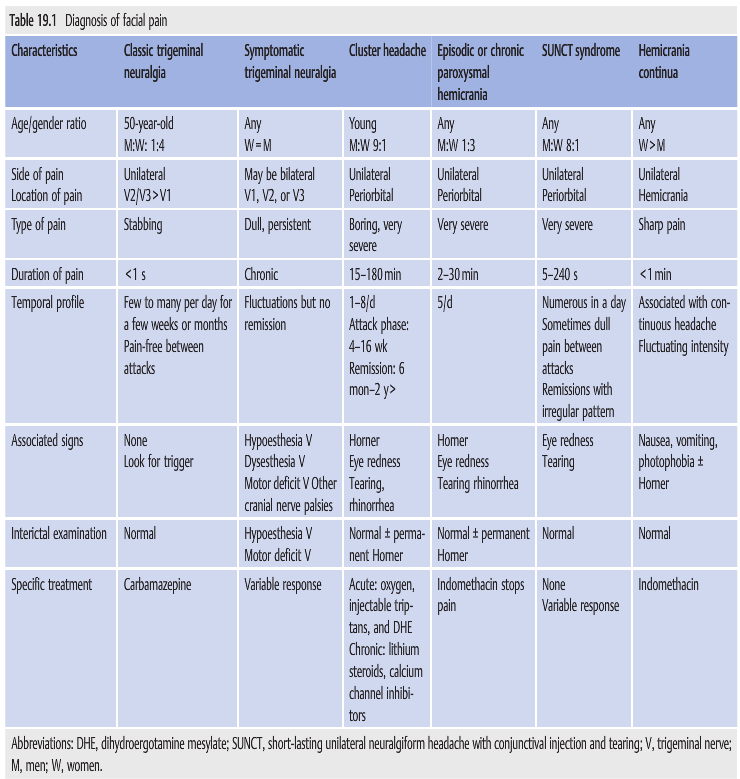
19.4 Differential Diagnosis of Facial Pain
▶Table 19.1 outlines the characteristics of various facial pain syndromes: classic trigeminal neuralgia, symptomatic trigeminal neuralgia, cluster headache, episodic or chronic paroxysmal hemicrania, SUNCT syndrome, and hemicrania continua. In most cases with new-onset facial pain or hemicrania, a workup is required to rule out underlying lesions (e.g., dissections, aneurysms, or cavernous sinus or skull base lesions).
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.