Questions: Transient monocular vision loss with:
1. Headache, scalp tenderness, jaw claudication, and diplopia suggest?
2. Eye or brow pain suggests?
3. Neck pain suggests?
4. Ipsilateral Horner syndrome suggests?
5. Simultaneous contralateral hemisensory or motor findings suggests?
6. Presyncope suggests?
7. When moving the eye suggests?
8. Blurry vision when reading suggests?
____________________________________________________
Answers: Transient monocular vision loss with:
1. Headache, scalp tenderness, jaw claudication, and diplopia suggest giant cell arteritis.
2. Eye or brow pain suggest intermittent angle closure glaucoma or giant cell arteritis.
3. Neck pain suggests cervical carotid artery dissection.
4. Ipsilateral Horner syndrome suggests carotid artery dissection.
5. Simultaneous contralateral hemisensory or motor findings suggest ipsilateral carotid artery stenosis.
6. Presyncope suggests systemic hypotension or a hyperviscosity syndrome.
7. When moving the eye suggests orbital mass.
8. Blurry vision when reading suggests dry eyes.
Explanation: “6.2.2 Patient Evaluation
The clinical history and a detailed ocular examination help determine the mechanism of the TMVL.
Among the first things to ask the patient about are the onset and duration of TMVL.
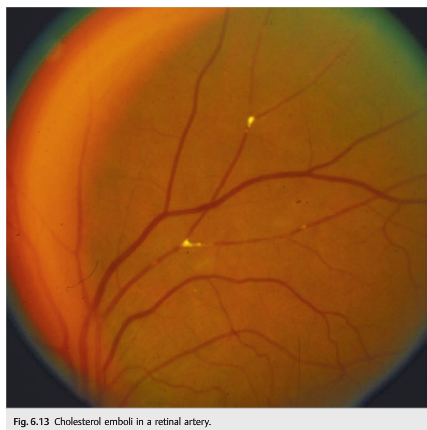
The answers can help determine the cause. For example, retinal emboli produce a very sudden TMVL, lasting from 1 to 4minutes. TMVL as a result of ocular hypoperfusion would be progressive, at least 5 to 10 minutes, and be precipitated by standing up or looking at bright lights. Venous congestion causes a progressive loss, lasting at least 10 to 20minutes. TVOs from optic nerve head anomalies are very brief, lasting only a few seconds, and are precipitated by bending over or by Valsalva maneuvers.
Accompanying manifestations helpful in determining the mechanism of TMVL include the following:
● Headache, scalp tenderness, jaw claudication, and diplopia: giant cell arteritis
● Eye or brow pain: intermittent angle closure glaucoma or giant cell arteritis
● Neck pain: cervical carotid artery dissection
● Ipsilateral Horner syndrome: carotid artery dissection
● Simultaneous contralateral hemisensory or motor findings: ipsilateral carotid artery stenosis
● Presyncope: systemic hypotension or a hyperviscosity syndrome
● TMVL when moving the eye: orbital mass
● Blurry vision when reading: dry eyes
The ocular examination can help to rule out local causes of TMVL and detect retinal emboli, retinal ischemia, venous stasis retinopathy, or evidence of optic nerve ischemia.
Eyes with a narrow anterior chamber angle may have episodes of angle closure glaucoma resolving spontaneously. During such episodes, the intraocular pressure is elevated, and patients complain of painful transient monocular blurry vision with the perception of halos around lights.”1
Reference:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.