From: MRI in the Evaluation of Acute Visual Syndromes.
Mukhi SV, Lincoln CM. Topics in Magnetic Resonance Imaging 24 (6):309-24. 2015
https://drive.google.com/open?id=1ayqCxDRn0E_Own4NkKoWbC2zqvfAc2X8
The prevalent use of antibiotics has decreased the overall incidence of CST. CST still carries significant mortality, commonly reported as approximately 30%, with more than 50% of the cases resulting in morbidity secondary to cranial neuropathies. CST is subclassified as aseptic or infectious in etiology. Aseptic causes include surgery or trauma. Infectious CST is typically a complication of a facial, orbital, odontogenic, or paranasal sinus infection. Sinusitis is the most common cause of CST, whereas odontogenic sources have been reported in up to 10% of the cases.3,33–39
The CS is a paired structure on either side of the sella, pituitary gland, and sphenoid sinus. It is composed of two layers of dura that are split to create a septate venous channel. The internal carotid artery (ICA) is the most medial structure and cranial nerves III, IV, and first and second branches of cranial nerve V are located in the lateral wall of the dura. Cranial nerve VI courses at the medial aspect of the ICA. Anteriorly, the CS is bordered by the SOF and OA. The posterior margin of the CS is immediately lateral to the dorsum sella and bordered by Meckel cave medially and the petrous apex posteroinferiorly.33,40,41
CST most commonly occurs secondary to the spread of infection by emissary veins as well as by direct extension. Emissary veins throughout the skull base are valve less and have bidirectional flow, accounting for the ease of contiguous spread.41 Spread of infection also occurs by the propagation of thrombus and/or septic embolism. It is postulated that bacteria stimulate the formation of thrombus by the release of a procoagulant substance and through toxins that cause tissue damage.38 In otitis media, infection spreads via the sigmoid sinus and along the internal carotid artery plexus. Staphylococcus aureus (70%) and Streptococcus sp (22%) are the important organisms responsible for infection of the CS. In patients with uncontrolled diabetes and immunocompromise, fungal infection can also be responsible, particularly mucormycosis.38,41
Tuberculosis has also been reported to cause both unilateral and bilateral CST; cavernous sinus tuberculoma may occur in the absence of pulmonary findings. Lymphomatous infiltration of the CS has been reported in both pediatric and adult patients.4
CST typically presents with orbital swelling, proptosis, chemosis, fever, and ophthalmoplegia. Visual impairment in CST has been reported in 7% to 22% of the cases, with blindness reported in 8% to 15% of the cases. As the disease progresses, decreased light perception and visual loss ensue. In a case report by Chen et al, CST-induced blindness suggested involvement of the bilateral retina and optic nerves. The postulated mechanisms accounting for visual impairment and blindness in CST include venous infarction of the retina and retinal ischemia caused by occlusion of either an ophthalmic artery branch or the central retinal artery, or by mechanical pressure at the OA.39
Chemosis, periorbital edema, and proptosis have been attributed to venous congestion.38 Papilledema as a result of raised intracranial pressure from a CST has been described as well.42 Palsies of III, IV, and VI cranial nerves secondary to compression result in impaired EOM motility. Intracranial extension of infection may result in meningitis, encephalitis, brain abscess, pituitary infection, epidural and subdural empyema, and coma/death.33,38,42
MRI is the radiologic examination of choice, and the CS should be imaged in its entirety. MRI demonstrates the contents of the CSs more effectively compared with CT.40 Imaging protocols should extend from the OA to the prepontine cistern. Routine T2, fluid-attenuated inversion recovery, and pre- and post-contrast T1 weighted images of the entire brain should be included. Postcontrast T1 weighted, 3-mm thick images should be obtained in the axial and coronal planes with at least one plane imaged utilizing a fat-saturation technique. Thin-section, postcontrast axial images may be acquired by three-dimensional spoiled gradient techniques. In addition, thin-section, three-dimensional, heavily T2 weighted images allow visualization of individual cranial nerves in the CS and adjacent cisterns.43 Pula et al describe the use of three-dimensional constructive interference in steady state to show smaller structures within the CS, making it the ideal choice to study cranial neuropathies in the CS.44
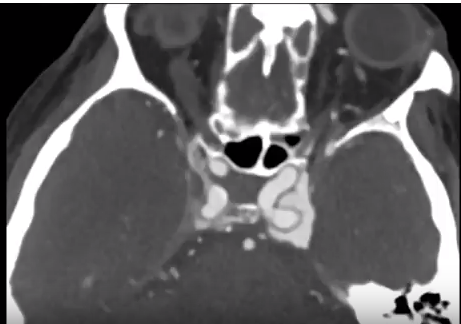
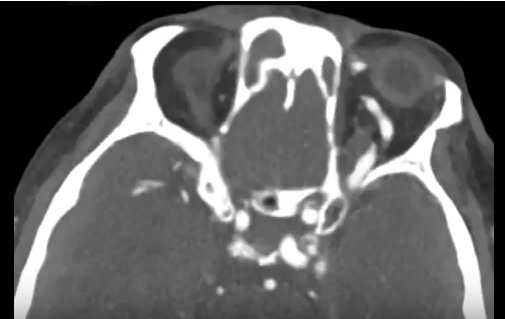
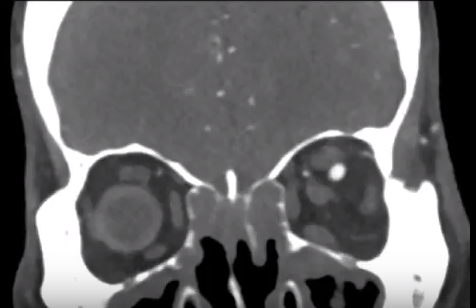
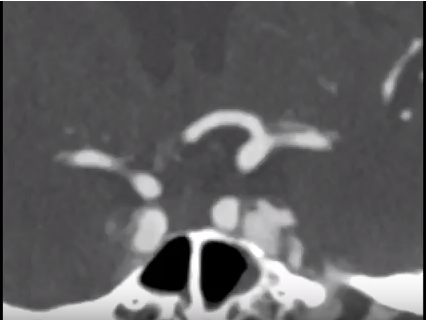
Alterations in signal intensity, size, and contour of the CS are subtle signs of thrombosis. A filling defect with enhancement of the peripheral margins of the CS suggests a clot within it (Fig. 4). Subacute thrombus exhibits high signal intensity on all pulse sequences, whereas acute thrombosis may appear more isointense. Indirect signs that may suggest the diagnosis are dilation of the superior ophthalmic veins, exophthalmos, and increased dural enhancement along the lateral border of CS and ipsilateral tentorium. Appropriate clinical symptoms, adjacent sinusitis, and orbital or odontogenic infection confirm the diagnosis and etiology.33,38,41,43
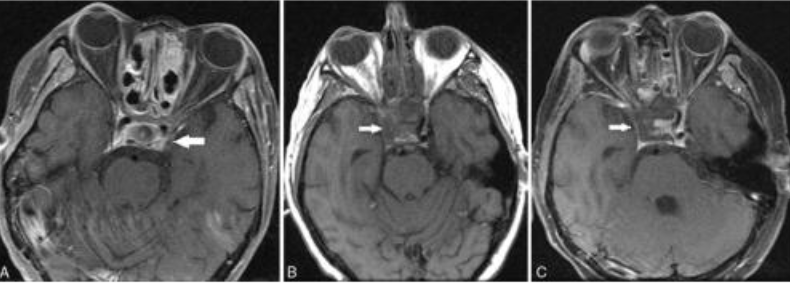
FIGURE 4. (A) Twenty-year-old man with invasive fungal sinusitis in setting of relapsed acute lymphocytic leukemia. Axial postcontrast image of the orbit and CS demonstrates filling defect in the left CS (arrow).
(B and C) Twenty-three-year old man with leukemia and rapidly progressive right-sided cranial neuropathy involving III, IV, and VI. Axial pre- (B) and post (C) contrast T1 images shows filling defect in the right CS with absence of the right cavernous carotid artery flow void (arrows).
CST therapy relies on mobilization of the varied disciplines of neurology, neurosurgery, otolaryngology, and infectious disease. Aggressive antibiotic therapy and surgical debridement of the primary site of infection and surrounding areas of involvement are the mainstay of treatment. The use of steroid therapy to reduce orbital edema and cranial nerve inflammation is controversial. Anticoagulant therapy has shown some benefit when initiated early.33,38,43