Teaching NeuroImages: The half-split man
Makoto Takahashi, Akiko Shinya, Hisao Kitazono, Teruhiko Sekiguchi, Akira Inaba, Satoshi Orimo. Neurology. September 13, 2016; 87 (11) RESIDENT AND FELLOW SECTION
ARTICLE
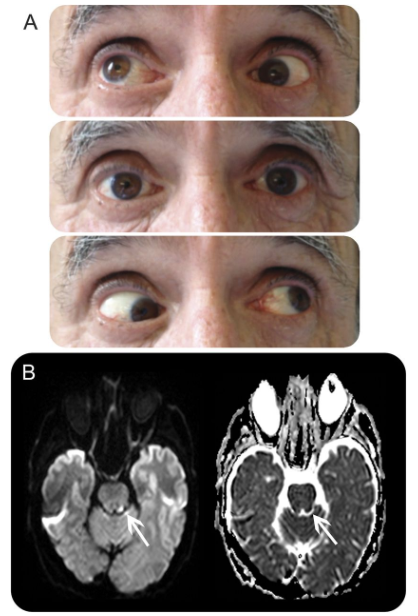
A 51-year-old man was admitted with left lateral medullary infarction due to vertebral artery dissection (figure 1). Neurologic examination revealed nystagmus, dissociated sensory disturbance, and no evidence of paralysis. Miosis and ptosis were observed on the ipsilateral side, but hypohidrosis was not apparent. Thermography revealed a bilateral discrepancy in body temperature, as if the patient were split down the middle (figure 2). Asymmetric skin temperature can occur among patients with Wallenberg syndrome associated with Horner syndrome due to a disturbance of the descending sympathetic tract that causes ipsilateral hypohidrosis and increased cutaneous blood flow.1

Figure 1 MRI and magnetic resonance angiography of the medulla and the vertebral artery
Diffusion-weighted and T2-weighted images show an acute infarction of the left lateral medulla (A, B). Magnetic resonance angiography and black-blood MRI show dissection of the left vertebral artery (C, D).
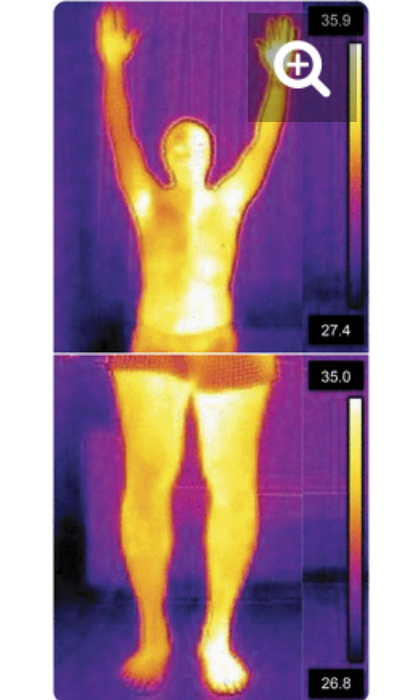
Figure 2 Thermography findings
Thermography images show the bilateral discrepancy in body temperature (in °C), as though the patient were split down the middle of his body.
AUTHOR CONTRIBUTIONS Dr. Takahashi: study concept, interpretation of data, and drafting the manuscript. Dr. Shinya: revision of the manuscript for intellectual content. Dr. Sekiguchi: study supervision. Dr. Kitazono: study supervision. Dr. Inaba: study supervision. Dr. Orimo: revision of the manuscript for intellectual content and study supervision.
STUDY FUNDING No targeted funding reported.
DISCLOSURE The authors report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
Footnotes Download teaching slides: Neurology.org
REFERENCE
1. Korpelainen JT, Sotaniemi KA, Myllylä VV. Asymmetrical skin temperature in ischemic stroke. Stroke 1995;26:1543–1547.