Unusual presentation of an Adie-like pupil Cat’s eye pupil
Robert A. Egan, Carla Avruskin
NEUROIMAGES
Neurology. 2018; 91 (15)
Article
A 55-year-old woman noticed that her right pupil was oddly shaped, associated with a mild ache. Her afferent visual examination, ocular and eyelid motility, and fundi were normal. Her left pupil was round and reactive (figure 1).

Figure 1 Close-up shows normal left pupil and tonic right cat’s eye pupil
The right pupil was elongated (points at 11:00 and 5:00) and tonic (figure 2).
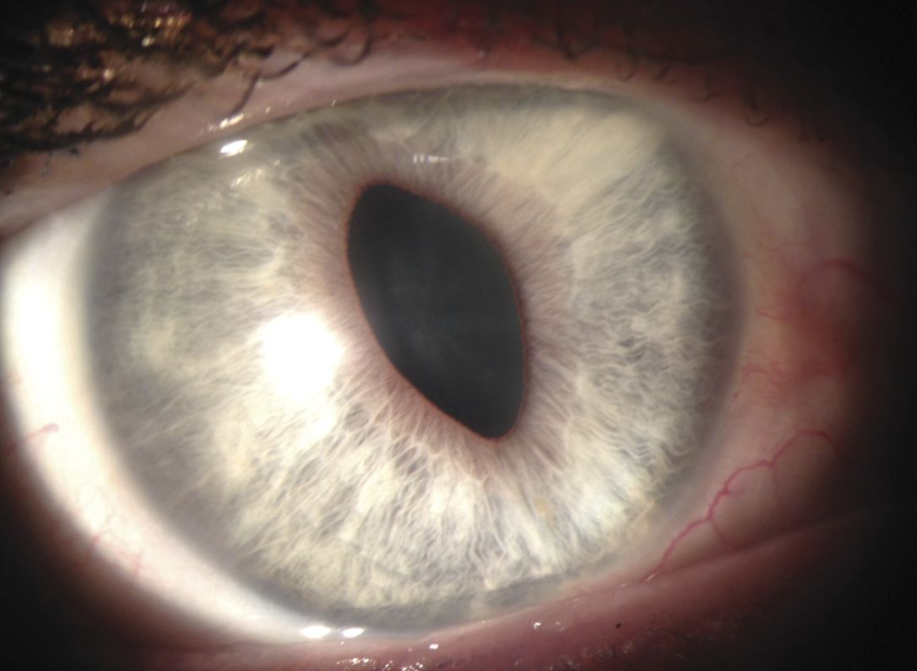
Figure 2 There was sectoral paralysis of the iris between 12:00 and 4:00 and also from 6:00 to 10:00 with mild thinning of the pupillary ruff on the temporal iris characteristic of an Adie-like pupil
There was no ocular hypertension or corneal edema. A year later, the pupil shape became triangular; evaluation revealed ocular hypertension without corneal edema, confirming the iridocorneal endothelial (ICE) syndrome. This case is an unusual presentation of a cat’s eye Adie-like pupil as the harbinger for ICE syndrome.