Recommended Reading – The clinical evaluation of infantile nystagmus: What to do first and why
The clinical evaluation of infantile nystagmus: What to do first and why.
Morgan Bertsch, Michael Floyd, Taylor Keohea, Wanda Pfeifer, and Arlene V. Dracka Ophthalmic Genet. 2017 ; 38(1): 22–33.
Department of Ophthalmology, Roy J. and Lucille A. Carver College of Medicine, University of Iowa, Iowa City, Iowa, USA
Abstract Introduction—Infantile nystagmus has many causes, some life threating. We determined the most common diagnoses in order to develop a testing algorithm.
Methods—Retrospective chart review. Exclusion criteria were no nystagmus, acquired after 6 months, or lack of examination. Data collected: pediatric eye examination findings, ancillary testing, order of testing, referral, and final diagnoses. Final diagnosis was defined as meeting published clinical criteria and/or confirmed by diagnostic testing. Patients with a diagnosis not meeting the definition were “unknown.” Patients with incomplete testing were “incomplete.” Patients with multiple plausible etiologies were “multifactorial.” Patients with negative complete workup were “motor.”
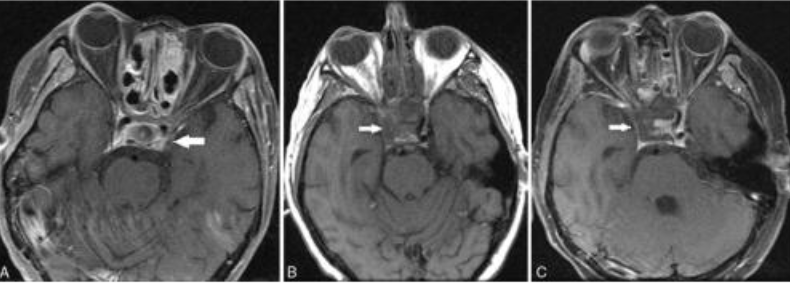
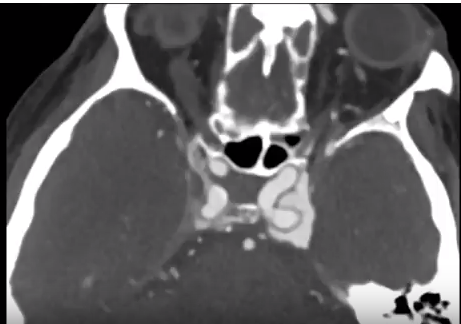
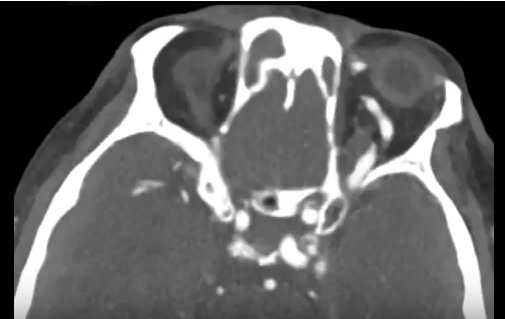
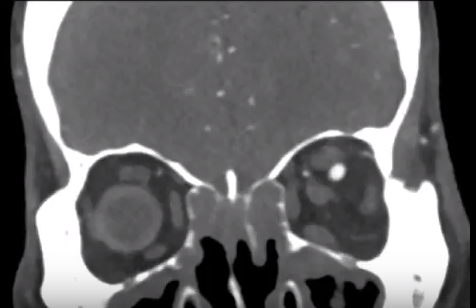
Results—284 charts were identified; 202 met inclusion criteria. The 3 most common causes were Albinism(19%), Leber Congenital Amaurosis(LCA)(14%) and Non-LCA retinal dystrophy (13%). Anatomic retinal disorders comprised 10%, motor another 10%. The most common first test was MRI (74/202) with a diagnostic yield of 16%. For 28 MRI-first patients, nystagmus alone was the indication; for 46 MRI-first patients other neurologic signs were present. 0/28 nystagmus-only patients had a diagnostic MRI while 14/46 (30%) with neurologic signs did. Yield of ERG as first test was 56%, OCT 55%, and molecular genetic testing 47%. 90% of patients had an etiology identified.
Conclusion—The most common causes of infantile nystagmus were retinal disorders (56%), however, the most common first test was brain MRI. For patients without other neurologic stigmata complete pediatric eye examination, ERG, OCT and molecular genetic testing had a higher yield than MRI scan. If MRI is not diagnostic, a complete ophthalmologic workup should be pursued.
Full Article https://drive.google.com/open?id=1h76ziIrxB6TpINMsPF1mcsWvvAvVkaj3