Recommended Reading – The expanding burden of idiopathic intracranial hypertension
The expanding burden of idiopathic intracranial hypertension
Susan P. Mollan, Magda Aguiar, Felicity Evison, Emma Frew & Alexandra J. Sinclair. Eye (2018)
Free Full Text: https://www.nature.com/articles/s41433-018-0238-5
Abstract
OBJECTIVE: To quantify the hospital burden and health economic impact of idiopathic intracranial hypertension.
METHODS: Hospital Episode Statistics (HES) national data was extracted between 1st January 2002 and 31st December 2016. All those within England with a diagnosis of idiopathic intracranial hypertension were included. Those with secondary causes of raised intracranial pressure such as tumours, hydrocephalus and cerebral venous sinus thrombosis were excluded.
RESULTS: A total of 23,182 new IIH cases were diagnosed. Fifty-two percent resided in the most socially deprived areas (quintiles 1 and 2). Incidence rose between 2002 and 2016 from 2.3 to 4.7 per 100,000 in the general population. Peak incidence occurred in females aged 25 (15.2 per 100,000). 91.6% were treated medically, 7.6% had a cerebrospinal fluid diversion procedure, 0.7% underwent bariatric surgery and 0.1% had optic nerve sheath fenestration. Elective caesarean sections rates were significantly higher in IIH (16%) compared to the general population (9%), p < 0.005. Admission rates rose by 442% between 2002 and 2014, with 38% having repeated admissions in the year following diagnosis. Duration of hospital admission was 2.7 days (8.8 days for those having CSF diversion procedures). Costs rose from £9.2 to £50 million per annum over the study period with costs forecasts of £462 million per annum by 2030.
CONCLUSIONS: IIH incidence is rising (by greater than 100% over the study), highest in areas of social deprivation and mirroring obesity trends. Readmissions rates are high and growing yearly. The escalating population and financial burden of IIH has wide reaching implications for the health care system.
Composite figure.
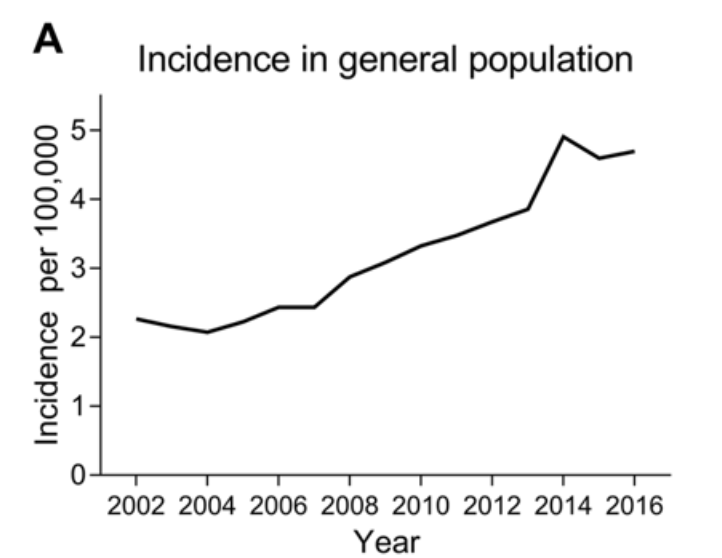
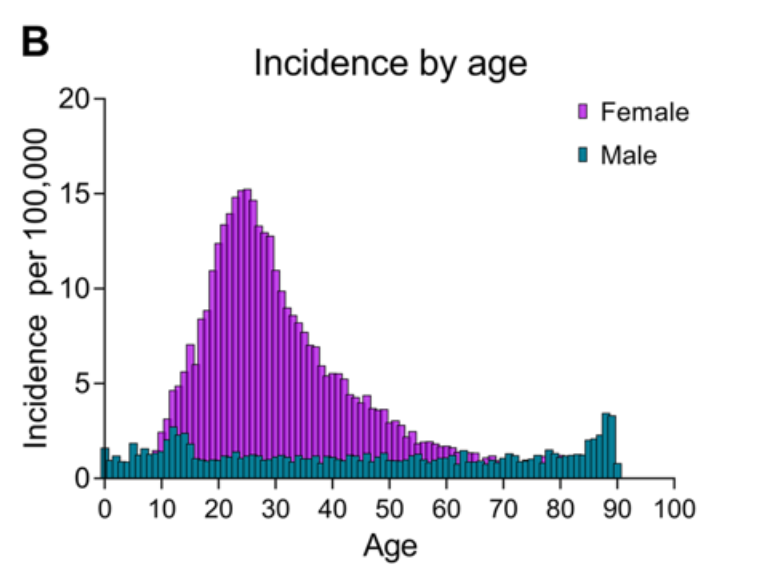
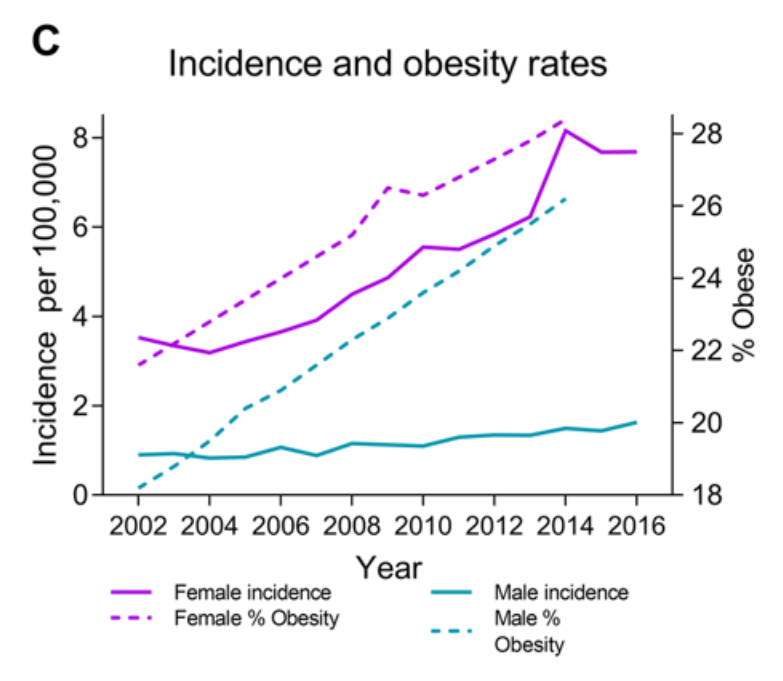
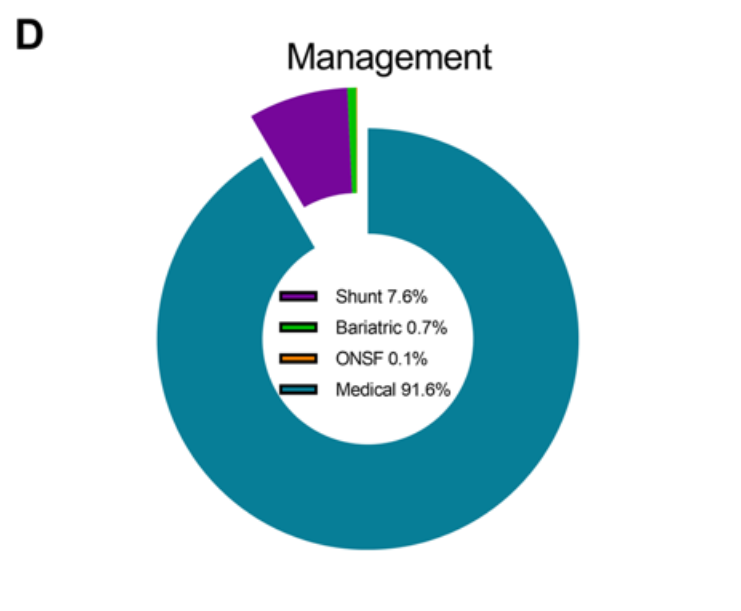
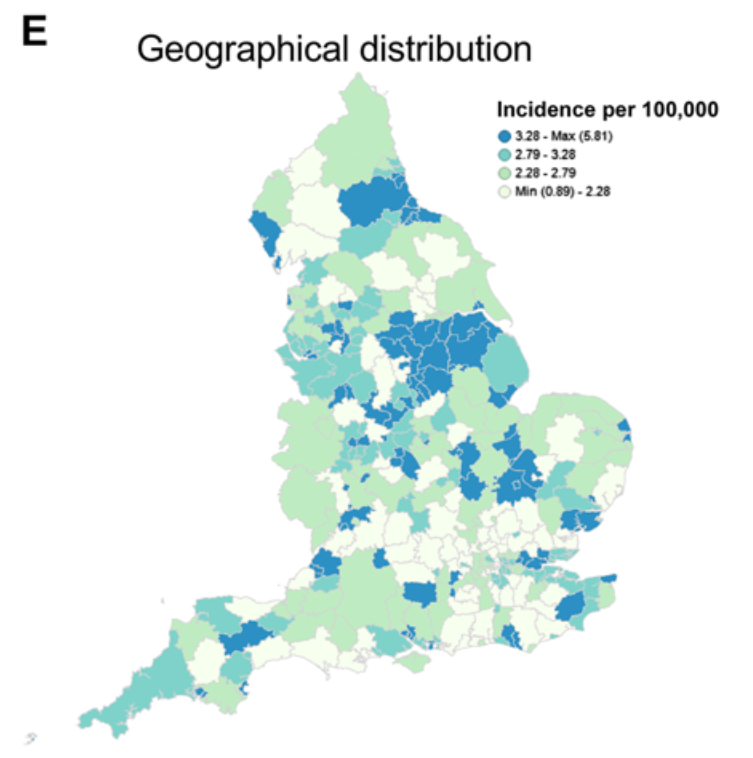
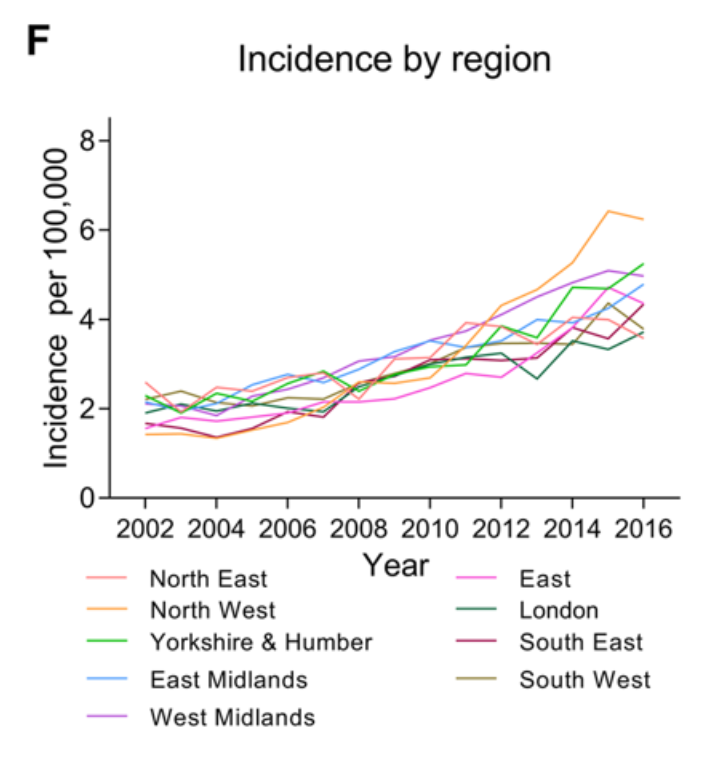
a Incidence in the general population. b Incidence by age and gender. c Annual incidence in females and males and Obesity rates (% obesity per annum (body mass index ≥ 30), age-standardized in 18 years + by gender in the United Kingdom. From World Health organisation http://apps.who.int/gho/data/node.main.A900A?lang=en Accessed 6 Oct 2017. d Management of IIH in the cohort. e Geographical distribution of diagnosed cases of IIH in England. F Distribution of cases by region per annum.