Recommended Reading – IMAGES IN CLINICAL MEDICINE Orbital Varix
Kiang L, Kahana A. N Engl J Med 2015; 372:e9v
A 63-year-old man was referred to our clinic with a 13-year history of intermittent vision loss, binocular diplopia, and blepharoptosis of the left eye during bending or straining that had worsened over the previous year. Other than uneventful cataract surgery, the patient had no clinically significant ocular history, and prior computed tomographic (CT) scans of the head and orbit did not identify any abnormality. An orbital vascular anomaly was suspected. A CT scan of the head was obtained while the patient performed the Valsalva maneuver, revealing the expansile orbital mass. On presentation to us, the patient’s visual acuity was 20/20 in the right eye and 20/50 in the left eye, with a relative afferent pupillary defect in the left eye. There was no proptosis on examination (Panel A).

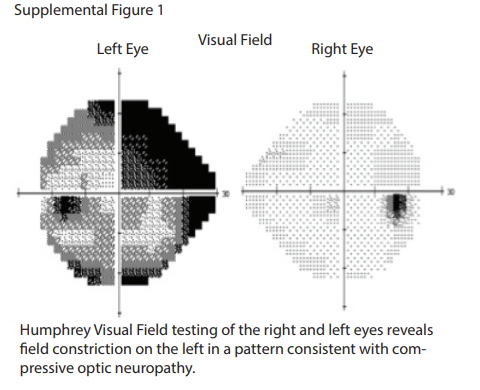
Visual-field testing revealed severe constriction.
A Valsalva maneuver induced 6 mm of proptosis in the left eye, with anterior superior globe displacement and blepharoptosis (Panel B, and video).


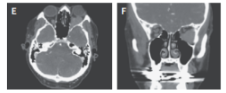
Proptosis quickly reversed on relaxation. CT of the orbit while the patient waw at at rest was unremarkable (Panels C and D show the axial and coronal views, respectively),
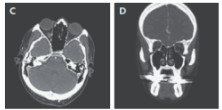
but a Valsalva maneuver revealed an orbital mass causing anterior superior globe displacement (Panels E and F).
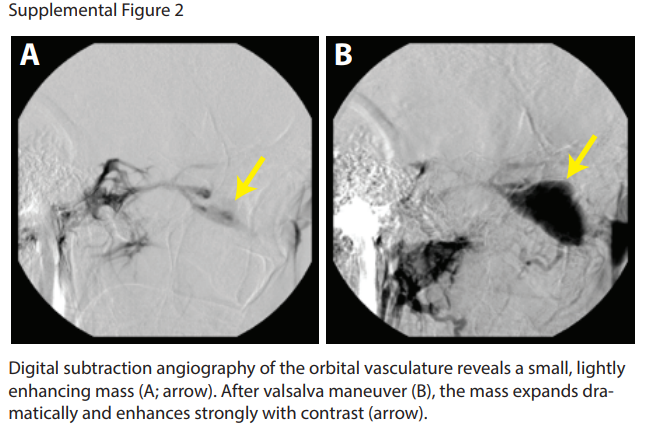
An orbital angiogram confirmed the presence of an expansile orbital mass (Fig. 2 in the Supplementary Appendix).
Although the differential diagnosis of an orbital mass is broad and includes lymphoma, metastatic tumors, and inflammatory masses, the clinical findings and imaging studies in this patient were pathognomonic of an orbital vascular anomaly and were most consistent with a distensible venous anomaly (i.e., varix). In the confines of the orbit, an expansile mass can cause intermittent orbital compartment syndrome and compressive optic neuropathy. The patient underwent successful endovascular and transorbital sclerosing treatment. The postoperative visual acuity was 20/30 in the left eye, with a stable visual field.