Question:
Which of the following are correct?
1. Heterochromia iridis in a child with Horner syndrome rules out neuroblastoma as a cause.
2. The most common cause of congenital Horner syndrome is a neuroblastoma.
3. Cervical neuroblastoma, a disease primarily of infants, has a favorable prognosis.
4. Cervical masses due to neuroblastoma, when felt, are commonly mistaken for infectious adenitis in children.
5. Cervical neuroblastoma in children almost always causes Horner syndrome.
 1
1
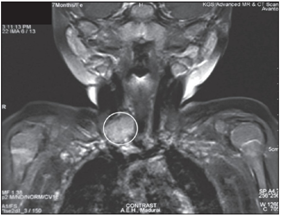
MRI showing a heterogeneously enhancing soft tissue lesion involving the root of neck
 2
2 1
1
 1
1 1
1 1
1 1
1 1
1