Question: Which of the following are required for anisocoria to be physiologic?
1. Both pupils must react briskly to light.
2. There must be no dilation lag 5-15 seconds after room illumination is reduced to near darkness.
3. The patient must not be aware of the anisocoria.
4. The anisocoria is 1 mm or less.
5. The anisocoria must be present on different days.
 1
1
__________________________________________
Correct Answers:
1. Both pupils must react briskly to light.
2. There must be no dilation lag 5-15 seconds after room illumination is reduced to near darkness.
4. The anisocoria is 1 mm or less.
Explanation:
“Anisocoria, or a difference in the diameter of the pupils in dim illumination, may be physiologic if the difference is less than 1 mm and both pupils react briskly and equally to light.”1
Physiologic Anisocoria
“Inequality of pupil size becomes clinically observable when the difference between pupils is about 3 mm. In dim light or darkness, almost 20% of the normal population hasan anisocoria of 0.4 mm or more at the moment of examination. In room light, this number drops to about 10%(112–114). This form of anisocoria is known by several names, including physiologic anisocoria, simple central anisocoria,essential anisocoria, and benign anisocoria. It is typically 0.6 mm or less; a difference in size of 1.0 or more is rare (114–116) (Fig. 16.6).
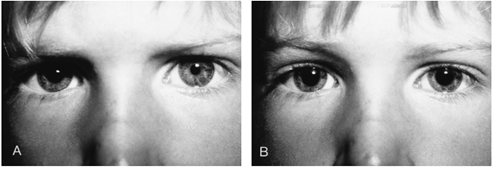 Figure 16.6. Physiologic (benign) anisocoria.
Figure 16.6. Physiologic (benign) anisocoria.
The degree of pupillary inequality in physiologic anisocoria may change from day today or even from hour to hour, however. The anisocoria usually diminishes slightly in bright light, perhaps because the smaller pupil reaches the zone of mechanical resistance first, giving the larger pupil a chance to make up the size difference (117).
Physiologic anisocoria is not caused by damage to the peripheral nerves that innervate the sphincter and dilator muscles of the iris. The pupillary reactions to light and darkness are normal. Instead, it is presumed to occur becausethe supranuclear inhibition of the parasympathetic pupilloconstrictornuclei in the midbrain is not balanced with anymore precision than is necessary for clear, binocular vision.It is unrelated to refractive error. Occasionally, a reversal of physiologic anisocoria is seen, a phenomenon termed ‘‘see saw anisocoria’’ (112,116).
When physiologic anisocoria is suspected, reviewing old photographs, such as a driver’s license or especially a family Figure 16.6. Physiologic (benign) anisocoria. The patient was a 5-year-old boy whose parents noted that the right pupil was larger than the other. The anisocoria was more obvious in dark than in light, and both pupils reacted normally to light stimulation.A, Appearance of the patient. Note anisocoria with right pupil larger than left. B, 45 minutes after instillation of a 10% solution of cocaine into both inferior conjunctival sacs, both pupils are dilated, indicating that anisocoria is not caused by sympathetic denervation. album, can be a valuable diagnostic tool (Fig. 16.7). In the latter case, the anisocoria usually can be traced back to infancy or early childhood.
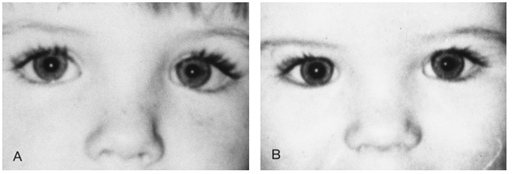
Value of old photographs in the assessment of anisocoria. A, This 3-year-old boy was noted by his parents to have intermittent anisocoria, with the right pupil larger than the left. The anisocoria was greater in darkness than in light, and both pupils reacted normally to light stimulation. B, Photograph of patient at age 7 months shows obvious anisocoria”2
Frequency of anisocoria
“We photographed the pupils of 128 normal subjects in dim light, morning and afternoon, for five consecutive days. Fifty-two of the subjects (41%) had an anisocoria of 0.4 mm or more at one time or another during these five days, but only four (3%) had unequal pupils of 0.4 mm or more in all ten photography sessions. At any given examination, a fairly constant 19% (24 of 128) of the subjects showed this amount of anisocoria. These numbers shifted dramatically when anisocoria was defined as a pupillary inequality of greater than, or less than, 0.4 mm. The prevalence of anisocoria did not vary with the time of day, from day to day, or from week to week, nor was it influenced by the sex, age, or iris color of the subject.”4
Videos
How to Examine the Normal Pupils – Tapsell S http://youtu.be/E2XzBaOOX8g
Anisocoria Examination. Tapsell S – https://www.youtube.com/watch?v=jgVJyEOXVvM
Physiologic Anisocoria. Tapsell S – https://www.youtube.com/watch?v=kzqgB2mPmGg&feature=c4-overview&list=UU7K3GgfCdrrvLRi3MiQOV4Q
Up-to-Date
 5
5
References:
1. Anisocoria. The Eyes Have It http://www.kellogg.umich.edu/theeyeshaveit/symptoms/anisocoria.html
2. Walsh and Hoyt’s Clinical Neuro-Ophthalmology 6th Edition. Miller NR, Newman NJ, Biousse V, Kerrison JB. 2005:1:3:16:749 Lippincott Williams & Wilkins http://content.lib.utah.edu/cdm/ref/collection/ehsl-wht/id/76
3. Horner’s Syndrome, Pseudo-Horner’s Syndrome, and Simple Anisocoria. Martin TJ, Current Neurology and Neuroscience Reports. 2007, 7:397–406
4. The prevalence of simple anisocoria. Lam BL, Thompson HS, Corbett JJ. Am J Ophthalmol. 1987;104(1):69.. Approach to the patient with anisocoria. Kedar S, Biousse V, Newman NJ. Up-to-Date. 2015
5. Approach to the patient with anisocoria. Kedar S, Biousse V, Newman NJ. Up-to-Date. 2015
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.