Question:
Which of the following are correct?
1. Heterochromia iridis in a child with Horner syndrome rules out neuroblastoma as a cause.
2. The most common cause of congenital Horner syndrome is a neuroblastoma.
3. Cervical neuroblastoma, a disease primarily of infants, has a favorable prognosis.
4. Cervical masses due to neuroblastoma, when felt, are commonly mistaken for infectious adenitis in children.
5. Cervical neuroblastoma in children almost always causes Horner syndrome.
 1
1
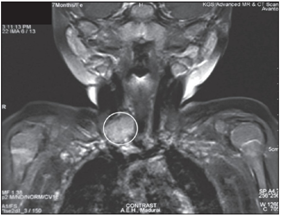
MRI showing a heterogeneously enhancing soft tissue lesion involving the root of neck
Answers:
3. Cervical neuroblastoma, a disease primarily of infants, has a favorable prognosis.
4. Cervical masses due to neuroblastoma, when felt, are commonly mistaken for infectious adenitis in children.
Explanation:
Pediatric Horner Syndrome: Etiologies and Roles of Imaging and Urine Studies to Detect Neuroblastoma and Other Responsible Mass Lesions.2
PURPOSE: To evaluate the frequency of etiologies of Horner syndrome in children and suggest an imaging and laboratory diagnostic protocol to evaluate for neuroblastoma and other lesions in a child presenting with Horner syndrome and no known cause.
DESIGN: Retrospective chart and data review.
METHODS: A retrospective review of all children seen at a large pediatric neuro-ophthalmology referral center with a diagnosis of Horner syndrome between 1993 and 2005 with particular attention to underlying etiologies and the results of imaging and urine catecholamine studies.
RESULTS: Fifty-six children met criteria for Horner syndrome and further review. Twenty-eight children (50%) had no previously identified cause for Horner syndrome. Of these children, 24 (85.7%) had urine catecholamine metabolite studies, and all had negative results. Twenty (71.4%) had complete modern imaging of the brain, neck, and chest. Of the 18 children who had complete imaging and urine studies, responsible mass lesions were found in six (33%). Four had neuroblastoma, one had Ewing sarcoma, and the other had juvenile xanthogranuloma. Of all patients (diagnosis known and unknown), neoplasm was the etiology in 13 of 56 (23%) of patients.
CONCLUSIONS: We confirm that Horner syndrome in a child of any age without a surgical history requires a complete examination to exclude a mass lesion. In such patients, we recommend brain, neck, and chest magnetic resonance imaging (MRI) with and without contrast as well as urinary catecholamine metabolite testing. However, imaging is more sensitive than urine testing in this setting.
Cervical neuroblastoma in eleven infants — a tumor with favorable prognosis. Clinical and radiologic (US, CT, MRI) findings. 3
“Cervical neuroblastoma, a disease primarily of infants, has a favorable prognosis. Eleven patients are reported. Clinical presentations (other than mass) included stridor and swallowing problems. Masses when felt were commonly mistaken for infectious adenitis. Imaging studies (US, CT, MRI) showed solid masses with vascular displacement and narrowing; intraspinal extension was absent though extension into the adjacent sites of mediastinum and skull occurred. Horner syndrome was seen in five patients with accompanying heterochromia iridis in one. Five tumors had calcification. A high index of suspicion will lead to biopsy and less delay in diagnosis once a mass is felt or imaged.”
Congenital or acquired Horner’s?1

Figure 1. Seven-month-old female baby with miosis, apparent enophthalmos of right eye and anhidrosis of right side of face
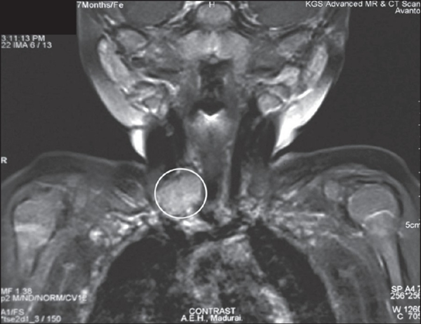
Figure 2. MRI of the neck showing a heterogeneously enhancing soft tissue lesion involving the root of neck
“The lesion was located close to or arising from the right sympathetic chain, which could have been either a lymph node or paraganglioma. The MRI of the thorax and abdomen was normal. Urine vanillylmandelic acid (VMA) assay yielded normal results excluding the possibility of neuroblastoma (32 micro moles/24h of urine) although there are varied reports on the reliability on this test since elevation of urine catecholamine mainly depends on tumor bulk.3 It was opined in consultation with the neurosurgeon to observe the progression and avoid biopsy since the lesion was very close to major vessel and had a high chance of hemorrhage.
Though brachial plexus injury is the most common cause of congenital HS, any lesion along the sympathetic chain may result in HS. Among these lesions, timely diagnosis of primary thoracic or cervical neuroblastoma is very crucial.”1
Heterochromia4
Heterochromia is classified primarily by its time of onset as either genetic (congenital, present at or shortly after birth) or acquired. Most cases of heterochromia are hereditary, and these may be associated with a congenital syndrome.
Other Signs5
“Anhidrosis: Variable degree of loss of sweating can be seen depending on the site of lesion. Central or preganglionic lesions tend to produce more noticeable anhidrosis. The sudomotor and vasomotor fibers to most of the face separate out at the superior cervical ganglion and anhidrosis is often not noticeable in postganglionic lesions.
Harlequin sign: Impaired hemi-facial (or hemi-body) flushing seen in children with sympathetic denervation to the face.
Cervical or abdominal mass may be seen in children with neuroblastoma.”
References:
1. Congenital or acquired Horner’s? Toprani K, Shetty S, Vijayalakshmi P. Indian J Ophthalmol. 200:5(5):399-400. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636023/figure/F2/
2. Pediatric Horner Syndrome: Etiologies and Roles of Imaging and Urine Studies to Detect Neuroblastoma and Other Responsible Mass Lesions. Mahoney NR, Liu GT, Shery LJ. Menacker SJ, Wilson MC, Hogarty MD, & Maris J, Md. Am J Ophthalmol 2006;142:651–659
3. Cervical neuroblastoma in eleven infants-a tumor with favorable prognosis. Clinical and radiologic (US, CT, MRI) findings. Abramson sJ, Berdon WE, Ruzal-Shapiro C, Stolar C & Garvin J. Pediatric radiology. 1993:23:4:253-257.
4. Heterochromia Iridis. Dahl AA, MedicineNet.com. 2016 http://www.medicinenet.com/heterochromia_iridis/page2.htm
5. Horner’s Syndrome. Burkat CN, Marcet MM, Kedar S & Kedar S. EyeWiki, AAO 2016 http://eyewiki.org/Horner’s_syndrome
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.