Questions:
1. Does a reduction in visual acuity due to a neurologic problem improve with the patient looking through a pinhole?
2. Can a reduction in the perceived brightness of a white light in one eye compared to the other be an early sign of optic nerve disease?
3. Can a reduction in the perceived saturation or brightness of colors in one eye compared to the other be an early sign of optic nerve disease?
4. Does a relative afferent pupillary defect ipsilateral to visual loss always indicate optic nerve dysfunction?
5. Does normal stereo vision indicate at least 20/20 visual acuity in each eye?
6. What level of vision does a positive response to the optokinetic nystagmus stimulus indicate?
7. What is the most common vascular cause of transient monocular visual loss?
8. What is amaurosis fugax?
9. What are 4 arteries in which reduced blood flow may cause amaurosis fugax?
Neuro-ophthalmology Illustrated Chapter 5 – Vision Loss: An Overview 1
Recommended Reading – Pupillary sign of aberrant regeneration of the third nerve
Recommended Reading – Pupillary sign of aberrant regeneration of the third nerve
Pupillary sign of aberrant regeneration of the third nerve
Olga R. Rosenvald, Simmons Lessell. Neurology. 2016; 86 (18)
VIDEO NEUROIMAGES
A 55-year-old woman presented with a third nerve palsy and impaired abduction of her right eye. MRI showed a lesion at the orbital apex extending into the cavernous sinus. A biopsy showed invasive Aspergillus fumigatus and she was treated with antifungals with only partial improvement.
Twelve years later, she had complete ptosis, partially restricted abduction, adduction, and depression of the right eye. The right pupil, which did not constrict to light or near vision, constricted on downgaze (video on the Neurology® Web site at Neurology.org), diagnostic of aberrant regeneration,1 which occurs when regenerating axons are misdirected to muscles they were not intended, such as the iris sphincter.2

Video https://drive.google.com/open?id=1D0qDczD0jsQ7q88eUL0KzVmMhlIOqqXf
The video shows a partial cranial nerve III palsy with a pupil reactive to neither light or near vision. However, the pupil constricts on attempted downgaze.
References:
1. Czarnecki JS, Thompson HS. The iris sphincter in aberrant regeneration of the third nerve. Arch Ophthalmol 1978;96:1606–1610.
2. Sibony PA, Lessell S, Gittinger JW. Acquired oculomotor synkinesis. Surv Ophthalmol 1984;28:382–390.
Neuro-ophthalmology Illustrated Chapter 4 – Ancillary Testing Commonly Used in Neuro-ophthalmology 3
18. What findings are likely to be present with ethambutol toxicity?
19. On MRI T1-weighted non-contrast images are each of the following structures hyperintense, or hypointense: fat, vitreous, CSF, subacute blood?
20. To improve the evaluation of orbital structures, what MRI techniques should be requested?
21. On MRI T2-weighted non-contrast images are the following structures hyperintense, or hypointense: fat, vitreous, CSF?
22. What special MRI sequence allows transformation of the bright CSF signal into a black signal while maintaining the other characteristics of a T2-weighted image?
23. What MRI technique is ideal for detecting acute cerebral ischemia?
24. What 5 techniques may be helpful in detecting optic nerve head drusen?
25. What MRI technique allows better visualization of blood products, such as hemosiderin?
26. What is Isodense on CT?
27. What is hypodense on CT?
28. What is hyperdense on CT?
29. What enhances with contrast on CT?
30. What are 7 good indications for CT?
31. What are 7 good indications for MRI?
Recommended Reading – Incidence and Causes of Overdiagnosis of Optic Neuritis.
Incidence and Causes of Overdiagnosis of Optic Neuritis.
Stunkel L, Kung NH, Wilson B, McClelland CM, Van Stavern GP.
JAMA Ophthalmol. 2018 Jan 1;136(1):76-81.
Abstract
IMPORTANCE: Diagnostic error is an important source of medical error. Overdiagnosis of optic neuritis may prompt unnecessary and costly diagnostic tests, procedures, and treatments.
OBJECTIVE: To assess the incidence of and characterize factors contributing to overdiagnosis of acute optic neuritis.
DESIGN, SETTING, AND PARTICIPANTS: In this retrospective clinic-based cross-sectional study of new patient encounters, 122 patients referred for acute optic neuritis at a university-based Midwestern neuro-ophthalmology clinic between January 2014 and October 2016 were studied. Data were analyzed from September 2016 to July 2017.
INTERVENTIONS: Definite diagnosis was determined by neuro-ophthalmologists. For patients with alterative diagnoses, the Diagnosis Error Evaluation and Research taxonomy tool was applied to categorize the type of diagnostic error.
MAIN OUTCOMES AND MEASURES: The primary outcome was the primary type of diagnostic error in patients erroneously diagnosed as having optic neuritis. Secondary outcomes included final diagnosis and interventions undergone prior to referral.
RESULTS: A total of 122 patients were referred with acute optic neuritis during the study period; 88 (72.1%) were female, and the mean (SD) age was 42.6 (14.0) years. Of these, 49 patients (40.2%; 95% CI, 31.4-49.4) were confirmed to have optic neuritis, and 73 (59.8%; 95% CI, 50.6-68.6) had an alternative diagnosis. The most common alternative diagnoses were headache and eye pain, functional visual loss, and other optic neuropathies, particularly nonarteritic anterior ischemic optic neuropathy. The most common diagnostic error was eliciting or interpreting critical elements of history, which occurred in 24 of 73 patients (33%) with alternative diagnoses. Other common errors included errors weighing or considering alternative diagnoses (23 patients [32%]), errors weighing or interpreting physical examination findings (15 patients [21%]), and misinterpreting diagnostic test results (11 patients [15%]). In patients with alternative diagnoses, 12 (16%) had normal magnetic resonance imaging findings preceding the referral, 12 (16%) had received a lumbar puncture, and 8 (11%) had received unnecessary treatment with intravenous steroids.
CONCLUSIONS AND RELEVANCE: These data suggest that nearly 60% (95% CI, 50.6-68.6) of patients referred for optic neuritis have an alternative diagnosis, with the most common errors being over reliance on a single item of history and failure to consider alternative diagnoses. Understanding pitfalls leading to overdiagnosis of optic neuritis may improve clinicians’ diagnostic process.
Free Full Text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5833602/
___________________________________________________
Medscape Commentary on Above Article
https://www.medscape.com/viewarticle/907024
Errors Abound in Diagnosing Optic Neuritis–How Can We Fix Them?
Brianne N. Hobbs, OD. January 03, 2019
Thinking about mistakes, especially medical mistakes, is uncomfortable. It is certainly more enjoyable to read about a promising new therapy than to scrutinize the reasons that medical mistakes are happening. Yet, medical mistakes are currently the third leading cause of death in the United States, and despite their prevalence, there is no systematic way of reporting such errors.[1]
Death is not the only adverse outcome of medical errors, and it is estimated that mistakes causing serious harm are 10-20 times more common than those causing lethal harm.[2] Misdiagnosis is one category of medical mistakes that may result in unnecessary referrals, procedures, and treatments. A seemingly simple way to deliver better care is to identify common mistakes and correct them. This process isn’t glamorous, but it is productive.
Focus on Optic Neuritis
In a recent study,[3] one large university-based neuro-ophthalmology clinic addressed the problem of misdiagnosis of optic neuritis. Over a 2-year period, the clinic received 122 referrals for optic neuritis. The records for each of these patients were examined retrospectively to determine whether the diagnosis of optic neuritis was accurate and, if not, the reasons that commonly led to misdiagnosis.
Alarmingly, 73 of the 122 patients referred to this center with a diagnosis of optic neuritis were actually misdiagnosed. This misdiagnosis rate of approximately 60% was consistent among all referral sources, including optometrists, ophthalmologists, and neurologists. The most common alternative diagnoses were headache with concurrent eye pain (22%), functional vision loss (19%), and other optic neuropathies (16%), including nonarteritic ischemic optic neuropathy (NAION; 12%). Patients older than 50 years were more likely to be misdiagnosed with optic neuritis.
The Path to Misdiagnosis
Why were so many patients misdiagnosed as having optic neuritis? The most common error was failure to interpret the critical elements of the history, which occurred in 33% of the patients. Specifically, an overreliance on a previous diagnosis of multiple sclerosis or optic neuritis led to inaccuracy in diagnosis. Additionally, too much emphasis was often given to eye pain or pain with eye movement, which was found in the referral notes of 29% of patients ultimately diagnosed with a different condition. Another source of diagnostic error was ignoring normal exam findings; the possibility of optic neuritis can almost be excluded entirely if the complete ocular examination is normal. Red cap desaturation testing was often given too much emphasis, resulting in the diagnosis of optic neuritis solely on one abnormal, subjective test.
Although the misdiagnosis of optic neuritis is not a lethal mistake, multiple patients received expensive and invasive procedures, such as MRI and lumbar punctures, which were not indicated. Eight patients were treated unnecessarily with IV steroids. Four patients diagnosed with optic neuritis actually had neoplasms. The cost of misdiagnosis was not death, but it did result in patient harm.
There are five major clinical applications of this study:
1. Optic neuritis almost always results in an abnormal MRI due to T2 hyperintensity or enhancement of the optic nerve; a normal MRI argues strongly against optic neuritis.
2. The presence of an afferent pupillary defect was strongly correlated with a true diagnosis of optic neuritis; only 21% of patients who had been documented as previously having normal pupillary testing were ultimately diagnosed with optic neuritis.
3. Pain upon eye movement is often caused by a headache with associated eye pain or visual disturbances and is not pathognomonic for optic neuritis.
4. NAION is often misdiagnosed as optic neuritis in elderly patients, even though NAION has a higher incidence in this demographic.
5. No single element of the case history should determine the diagnosis, as this leads to diagnosis bias and a failure to consider other possible diagnoses.
Atul Gawande, in his book Complications: A Surgeon’s Notes on an Imperfect Science,[4] writes that “not only do all human beings err, but they err frequently and in predictable patterned ways.” Gathering data about these “predictable patterned ways” that clinicians err would help describe the scope of the problem, identify specific cognitive biases that lead to misdiagnosis, and generate explicit recommendations to improve patient care.
While this study was small and limited in scope, the methodology has broad applicability in enhancing patient care by reducing medical mistakes.
References:
1. Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016;353:i2139.
2. James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9:122-128.
3. Stunkel L, Kung NH, Van Stavern GP. Incidence and causes of overdiagnosis of optic neuritis: physician insecurity-reply. JAMA Ophthalmol. 2018;136:1312-1313.
4. Gawande A. Complications: A Surgeon’s Notes on an Imperfect Science. New York, NY: Picador; 2002.
Neuro-ophthalmology Illustrated Chapter 4 – Ancillary Testing Commonly Used in Neuro-ophthalmology 2
Questions:
11. What causes autofluorescence in the fundus?
12. What are the abnormal states of lipofuscin?
13. Do optic nerve drusen cause hyperautofluorescence or hypoautofluorescence?
14. Fluorescein angiography can help differentiate macular from optic nerve related visual loss. True or False?
15. Demonstration of retinal small vessel vasculopathy such as vasculitis is best done with retinal fluorescein angiography. True or False?
16. How is ultrasound helpful in assessing papilledema/pseudopapilledema?
17. What are 7 indications for B-scan echography?
Neuro-ophthalmology Illustrated Chapter 4 – Ancillary Testing Commonly Used in Neuro-ophthalmology 1
Questions:
1. The visual evoked response is not accurate if the patient fails to cooperate. True or False?
2. The visual evoked response is primarily a function of central visual function. True or False?
3. Visual evoked responses are most useful in evaluating the integrity of the visual pathway in infants and inarticulate adults. True or False?
4. In optic neuropathy, the ERG should be normal. True or False?
5. Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss. True or False?
6. The ERG is invariably severely depressed by the time patients complain of visual loss due to retinal disease. True or False?
7. Can a patient substantially alter the full-field ERG voluntarily?
8. Can a patient substantially alter the multifocal ERG voluntarily?
9. Multifocal ERGs are extremely helpful in detecting occult focal retinal abnormalities within the macula. True or False?
10. The multifocal ERG simultaneously records locations within the central 30 degrees. True or False?
Recommended Reading – Optical coherence tomography is a useful tool in the differentiation between true edema and pseudoedema of the optic disc.
Recommended Reading – Optical coherence tomography is a useful tool in the differentiation between true edema and pseudoedema of the optic disc.
Optical coherence tomography is a useful tool in the differentiation between true edema and pseudoedema of the optic disc.
PLoS One. 2018 Nov 29;13(11):e0208145. Carta A, Mora P, Aldigeri R, Gozzi F, Favilla S, Tedesco S, Calzetti G, Farci R, Barboni P, Bianchi-Marzoli S, Fossarello M, Gandolfi S1, Sadun AA.
Abstract
PURPOSE: To assess the usefulness of spectral-domain optical coherence tomography (SD-OCT) peripapillary retinal nerve fiber layer (RNFL) thickness measurement in discriminating early phase optic disc edema (ODE) from pseudoedema (PODE).
METHODS: Hospital-based, multicenter, cross-sectional study involving external patients referred for recent identification of “presumed ODE”. Patients underwent SD-OCT optic nerve head (ONH) RNFL thickness measurement at their first evaluation. In 155 of these, the causative etiology was subsequently ascertained and the respective eyes (one per patient) were assigned to the ODE (95 eyes) or PODE (60 eyes) group. Admission SD-OCT data were retrieved and used for the analysis. ROC curve analysis was used to calculate specificity, sensitivity and predictive value (PV) of the RNFL values.
RESULTS: The PODE group was significantly younger than the ODE group (p = 0.007). The average and any single-quadrant RNFL thickness was significantly higher in the ODE group compared with the PODE and control groups. The average and the inferior quadrant thicknesses tested the most powerful parameters to differentiate ODE from PODE. A cutoff value of ≥ 110 μm for the average area, or of ≥ 150 μm for the inferior quadrant was associated with maximal sensitivity and specificity with positive PV greater than 80%.
CONCLUSIONS: The SD-OCT evaluation of the peripapillary RNFL achieved good specificity, sensitivity and positive PV in discriminating between ODE and PODE. Despite the correct differential diagnosis between these categories still relies on a careful medical history taking and other ancillary testing, we proved the usefulness of SD-OCT RNFL measurement in supporting the diagnostic process.
Free Full Text https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6264818/
Recommended Reading – Diagnostic Errors in Initial Misdiagnosis of Optic Nerve Sheath Meningiomas
Recommended Reading – Diagnostic Errors in Initial Misdiagnosis of Optic Nerve Sheath Meningiomas
Diagnostic Errors in Initial Misdiagnosis of Optic Nerve Sheath Meningiomas
Pinar Kahraman-Koytak, MD; Beau B. Bruce, MD, PhD; Jason H. Peragallo, MD; Nancy J. Newman, MD; Valérie Biousse, MD. JAMA Neurol. Published online December 17, 2018.
IMPORTANCE Diagnostic errors can lead to the initial misdiagnosis of optic nerve sheath meningiomas (ONSM), which can lead to vision loss.
OBJECTIVE To identify factors contributing to the initial misdiagnosis of ONSM.
DESIGN, SETTING, AND PARTICIPANTS We retrospectively reviewed 35 of 39 patients with unilateral ONSM (89.7%) who were seen in the tertiary neuro-ophthalmology practice at Emory University School of Medicine between January 2002 and March 2017. The Diagnosis Error Evaluation and Research taxonomy tool was applied to cases with missed/delayed Diagnoses.
EXPOSURES Evaluation in a neuro-ophthalmology clinic.
MAIN OUTCOMES AND MEASURES Identifying the cause of diagnostic errors for patients who initially received a misdiagnosis who were found to have ONSM.
RESULTS Of 35 patients with unilateral ONSM (30 women [85.7%]; mean [SD] age, 45.26 [15.73] years), 25 (71%) had a diagnosis delayed for a mean (SD) of 62.60 (89.26) months. The most common diagnostic error (19 of 25 [76%]) was clinician assessment failure (errors in hypothesis generation and weighing), followed by errors in diagnostic testing (15 of 25 [60%]). The most common initial misdiagnosis was optic neuritis (12 of 25 [48%]), followed by the failure to recognize optic neuropathy in patients with ocular disorders. Five patients who received a misdiagnosis (20%) underwent unnecessary lumbar puncture, 12 patients (48%) unnecessary laboratory tests, and 6 patients (24%) unnecessary steroid treatment. Among the 16 patients who initially received a misdiagnosis that was later correctly diagnosed at our institution, 11 (68.8%) had prior magnetic resonance imaging (MRI) results that were read as healthy; 5 (45.5%) showed ONSM but were misread by a non-neuroradiologist and 6 (54.5%) were performed incorrectly (no orbital sequence or contrast). Sixteen of the 25 patients (64%) had a poor visual outcome.
CONCLUSIONS AND RELEVANCE Biased preestablished diagnoses, inaccurate funduscopic examinations, a failure to order the correct test (MRI brain/orbits with contrast), and a failure to correctly interpret MRI results were the most common sources of diagnostic errors and delayed diagnosis with worse visual outcomes and increased cost (more visits and tests). Easier access to neuro-ophthalmologists, improved diagnostic strategies, and education regarding neuroimaging should help prevent diagnostic errors.
Full Text: https://drive.google.com/open?id=1sZB52iNgoN7LdAkT0rMDeB6tc6WsL9zM
Neuro-ophthalmology Illustrated Chapter 3 – Visual Fields
Questions:
1. What values indicate an unreliable Humphrey Visual Field?
2. What are the monocular VF defect patterns?
3. What are the bilateral VF defect patterns?
4. A lesion of Wilbrand’s Knee results in what visual field defect?
5. What is the visual field defect of a junctional scotoma?
6. Where is the lesion of a junctional scotoma?
7. What are the findings of a left optic tract lesion?
8. What are the findings of a temporal lobe lesion?
9. What are the findings of a parietal lobe lesion?
10. What are the findings of an occlusion of the posterior cerebral artery?
11. What field defects results from ischemia limited to of the tip of an occipital lobe?
12. What field defect results when a stroke affects the occipital lobe but spares the anterior portion of the occipital lobe?
13. What field defect results when a stroke only affects the anterior portion of the occipital lobe?
14. What are the findings of bilateral occipital lobe lesions?
15. In interpreting a visual field test, what questions should be asked?
Recommended Reading – Neuro-ophthalmological manifestations of Behçet’s disease
Recommended Reading – Neuro-ophthalmological manifestations of Behçet’s disease
Neuro-ophthalmological manifestations of Behçet’s disease
Ammr Alghamdi, Bahram Bodaghi, Chloé Comarmond, Anne Claire Desbois, Fanny Domont, Bertrand Wechsler, Raphael Depaz, Phuc Le Hoang, Patrice Cacoub, Valérie Touitou, David Saadoun
British Journal of Ophthalmology. 2018
Abstract
Background The neuro-ophthalmological manifestations of Behcet’s disease (BD) are rare, and data regarding their characteristics and outcome are lacking.
Objective To report prevalence, main characteristics and outcome of neuro-ophthalmological manifestations in BD.
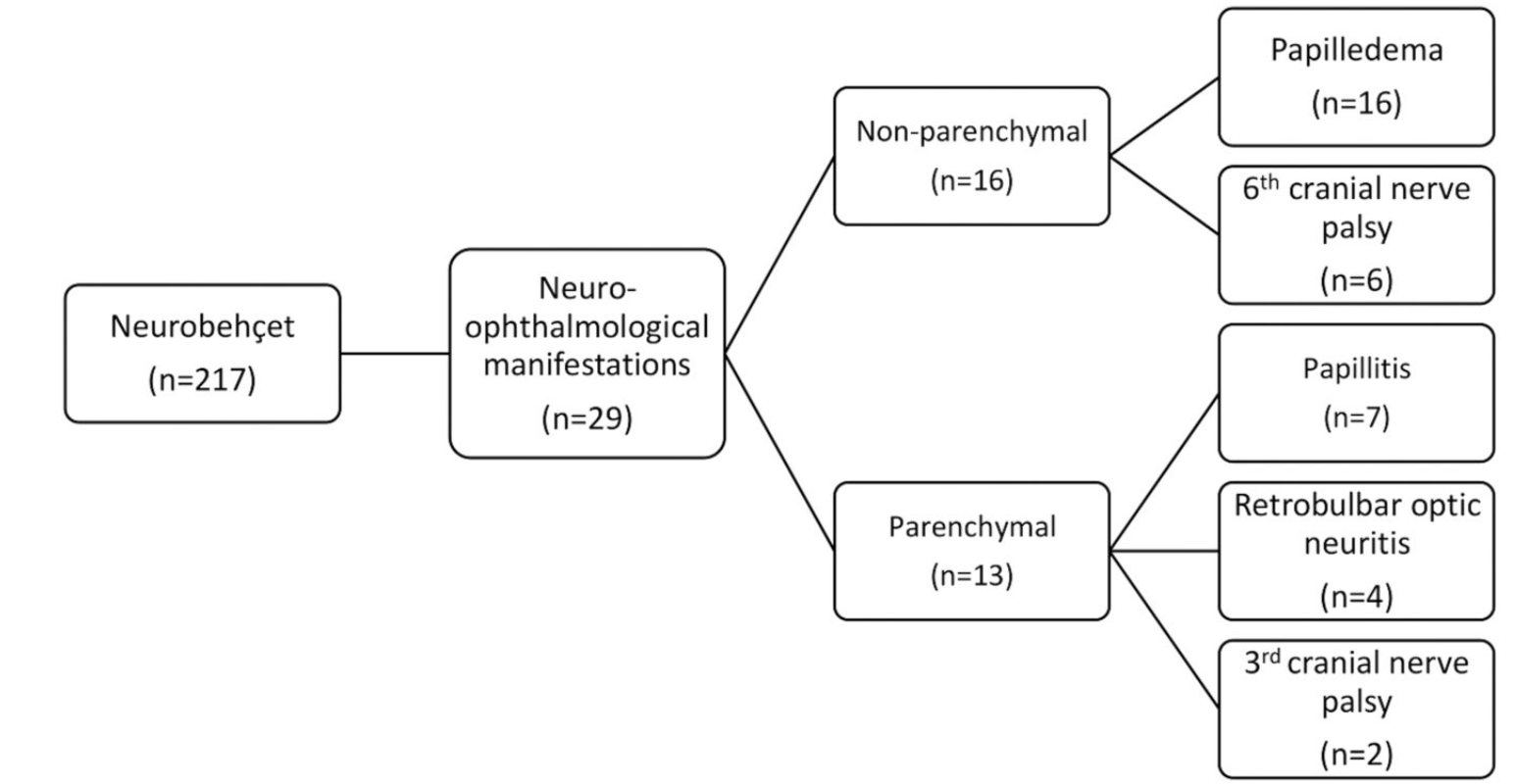
Patients and methods This is a retrospective monocentric study of 217 patients diagnosed with neuro-Behçet’s disease (NBD), of whom 29 (13.3%) patients presented with neuro-ophthalmological manifestations (55% of men and mean±SD age of 26±8 years). All patients underwent a detailed ophthalmological examination and were followed up in the internal medicine and the ophthalmology departments.
Results Neuro-ophthalmological manifestations were the first presentation of BD in 45% of patients and developed later in the course of the disease in 55% of patients. They are divided into parenchymal (PM) and non-parenchymal (NPM)-related manifestations in, respectively, 13 patients (45%) and 16 patients (55%). PM included papillitis in seven patients (53.8%), retrobulbar optic neuritis in four patients (30.8%) and third cranial nerve palsy in two patients (15.4%). NPM included papilloedema related to cerebral venous thrombosis in all 16 patients, of whom 6 patients (37.5%) had sixth cranial nerve palsy. At initial examination, 93.1% of patients had visual alterations, including mainly decreased visual acuity visual field defects and/or diplopia. All patients were treated with corticosteroids and 79% of patients received immunosuppressive agents. After treatment, the visual outcome improved or stabilised in 66.7% of patients while it worsened in 33.3. The mean±SD logarithm of the minimum angle of resolution visual acuity improved from 0.4±0.3 at diagnosis to 0.2±0.3 after therapy. 10.3% and 3.4% of patients were legally blind at diagnosis and after therapy, respectively.
Conclusion Neuro-ophthalmological manifestations of BD represented 13% of NBD. They could be potentially severe and disabling. Prompt treatment is the key factor in improving visual outcome.
Full Text https://drive.google.com/file/