Questions:
1. What values indicate an unreliable Humphrey Visual Field?
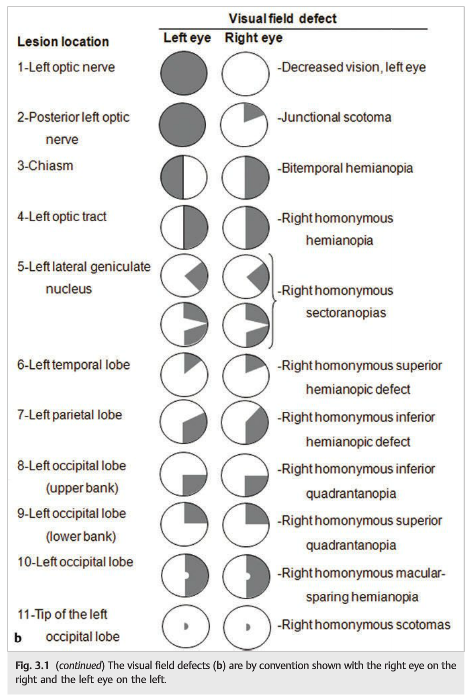
2. What are the monocular VF defect patterns?
3. What are the bilateral VF defect patterns?
4. A lesion of Wilbrand’s Knee results in what visual field defect?
5. What is the visual field defect of a junctional scotoma?
6. Where is the lesion of a junctional scotoma?
7. What are the findings of a left optic tract lesion?
8. What are the findings of a temporal lobe lesion?
9. What are the findings of a parietal lobe lesion?
10. What are the findings of an occlusion of the posterior cerebral artery?
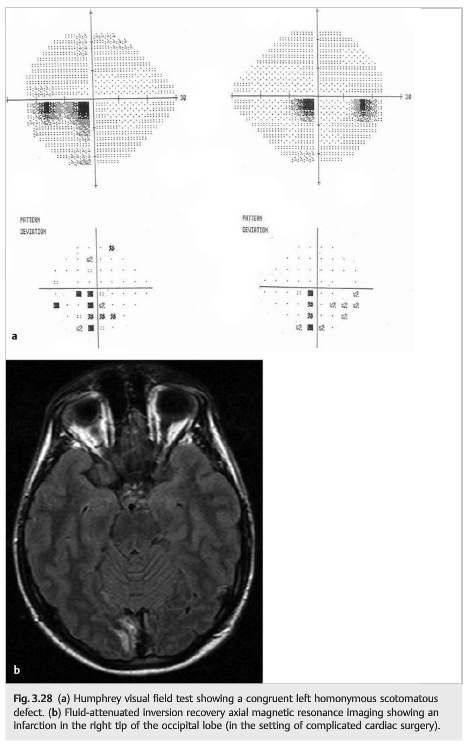
11. What field defects results from ischemia limited to of the tip of an occipital lobe?
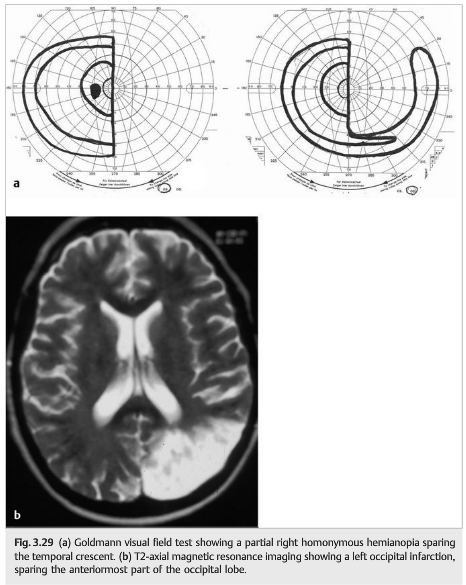
12. What field defect results when a stroke affects the occipital lobe but spares the anterior portion of the occipital lobe?
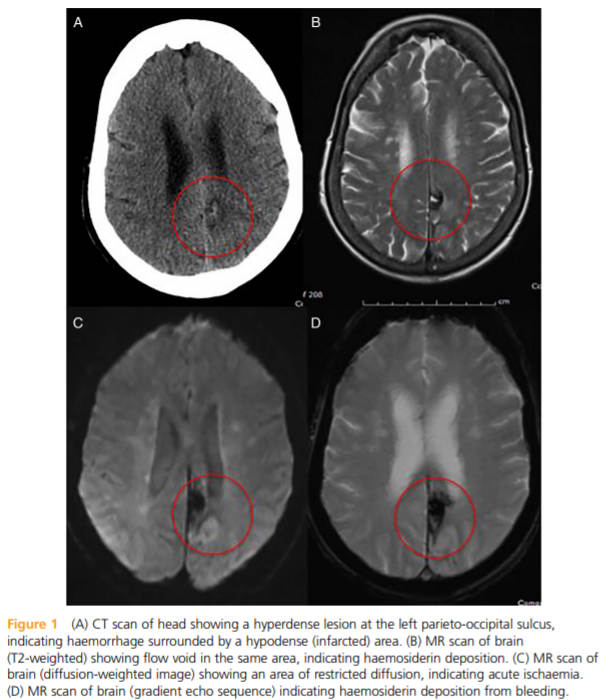
13. What field defect results when a stroke only affects the anterior portion of the occipital lobe?
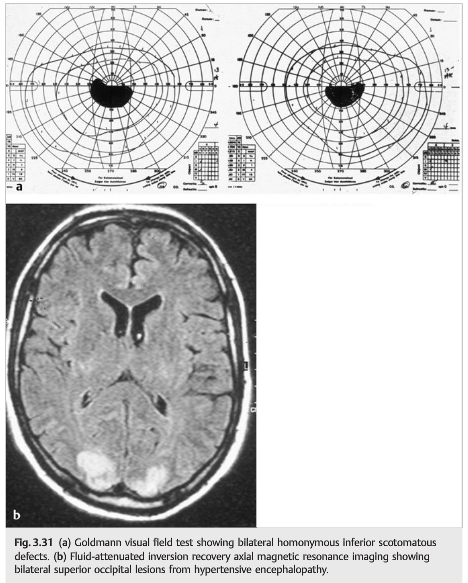
14. What are the findings of bilateral occipital lobe lesions?
15. In interpreting a visual field test, what questions should be asked?
_____________________________________________________
Questions with answers:
1. What values indicate an unreliable Humphrey Visual Field?
Rates must be under:
1. Fixation Loss 20%
2. False Negative 33%
3. False Positive 33%.
2. What are the monocular VF defect patterns?
Central, Cecocentral, Paracentral, Arcuate/Sector, Nasal Step, Altitudinal, Enlarged blind spots, Temporal Crescent Defect.
3. What are the bilateral VF defect patterns?
Junctional scotoma, Bitemporal defects, Homonymous hemianopia defects (w/wo macular sparing, spared temporal crescent)
4. A lesion of Wilbrand’s Knee results in what visual field defect?
A junctional scotoma. Wilbrand’s knee is composed of fibers originating in the inferonasal retina which after traversing via the optic nerve and crossing in the chiasm go anteriorly into the contralateral optic nerve up to 4 mm before passing posteriorly to the optic tract.
5. What is the visual field defect of a junctional scotoma?
A central scotoma in the eye ipsilateral to the lesion & a superotemporal defect in the fellow eye.
6. Where is the lesion of a junctional scotoma?
The lesion is at the most posterior portion of the optic nerve ipsilateral to the central scotoma at its “junction” with the chiasm.
7. What are the findings of a left optic tract lesion?
1. A right homonymous hemianopia (contralateral to lesion)
2. A right RAPD (contralateral to lesion) because more fibers (53%) in the optic tract come from the opposite eye’s nasal retina, having crossed in the chiasm.
3. Bowtie atrophy of the right optic nerve from atrophy of fibers supplying the nasal half of the macula and nasal retina of the right eye.
4. Mostly temporal pallor of the left optic nerve from atrophy of the temporal retina in the left eye.
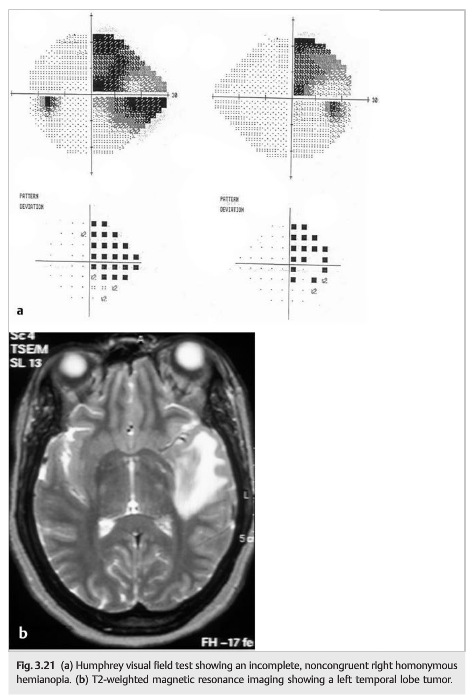
8. What are the findings of a temporal lobe lesion?
1. A Homonymous hemianopia denser superiorly (“pie in the sky”)
2. a normal, symmetrical OKN response.
9. What are the findings of a parietal lobe lesion?
1. A homonymous hemianopsia denser inferiorly (opposite of pie in the sky)
2. Deep lesions of the parietal lobe often impair optokinetic nystagmus when stimuli are moved in the direction of the damaged parietal lobe.
10. What are the findings of an occlusion of the posterior cerebral artery?
Occlusion of the PCA often results homonymous hemianopia of the contralateral visual field with macular sparing. The tip of the occipital lobe, where the macular central homonymous hemifields are represented, often has a dual blood supply from terminal branches of the posterior cerebral artery and of the middle cerebral artery. If the middle cerebral artery is patent when the PCA is occluded, this focal area of the occipital lobe may be spared.
11. What field defects results from ischemia limited to of the tip of an occipital lobe?
A contralateral homonymous hemianopia that is small and centrally located. An embolic infarction of either a distal MCA or PCA branch can result in exclusive ischemia of the tip of the occipital lobe, thereby producing only a small homonymous hemianopia if there is inadequate collateral circulation.
12. What field defect results when a stroke affects the occipital lobe but spares the anterior portion of the occipital lobe?
The VF defect is a homonymous hemianopia with sparing of the temporal crescent on the same side as the hemianopia.
13. What field defect results when a stroke only affects the anterior portion of the occipital lobe?
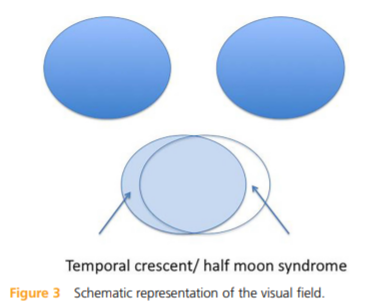
Retrochiasmal lesions normally cause homonymous visual field defects; the only exception is the ‘temporal crescent’ or ‘half moon syndrome’, caused by a lesion in the anterior part of the contralateral parieto-occipital sulcus.
The most nasal retinal fibers have unpaired cortical representation, which is situated in the most anterior part of the contralateral parieto-occipital sulcus. Thus the nasal visual field extends to 60% of the horizon, whereas the temporal field extends to a further 30°-40°
14. What are the findings of bilateral occipital lobe lesions?
1. Bilateral homonymous hemianopias
2. Possibly a decreased visual acuity that is equal in each eye (unless additional pathology is present anterior to chiasm).
15. In interpreting a visual field test, what questions should be asked?
1. Is the test reliable (as indicated by the technician for Goldmann visual fields and by the reliability parameters for automated perimetry)?
2. Is the test normal?
3. Does the visual field defect involve one eye or two eyes?
4. If binocular, does the defect respect the vertical meridian?
5. If it respects the vertical meridian, is the defect bitemporal or homonymous?
6. If it is homonymous, is the defect complete or incomplete?
7. If it is homonymous and incomplete, is the defect congruent (same defect shape and size in each eye)?
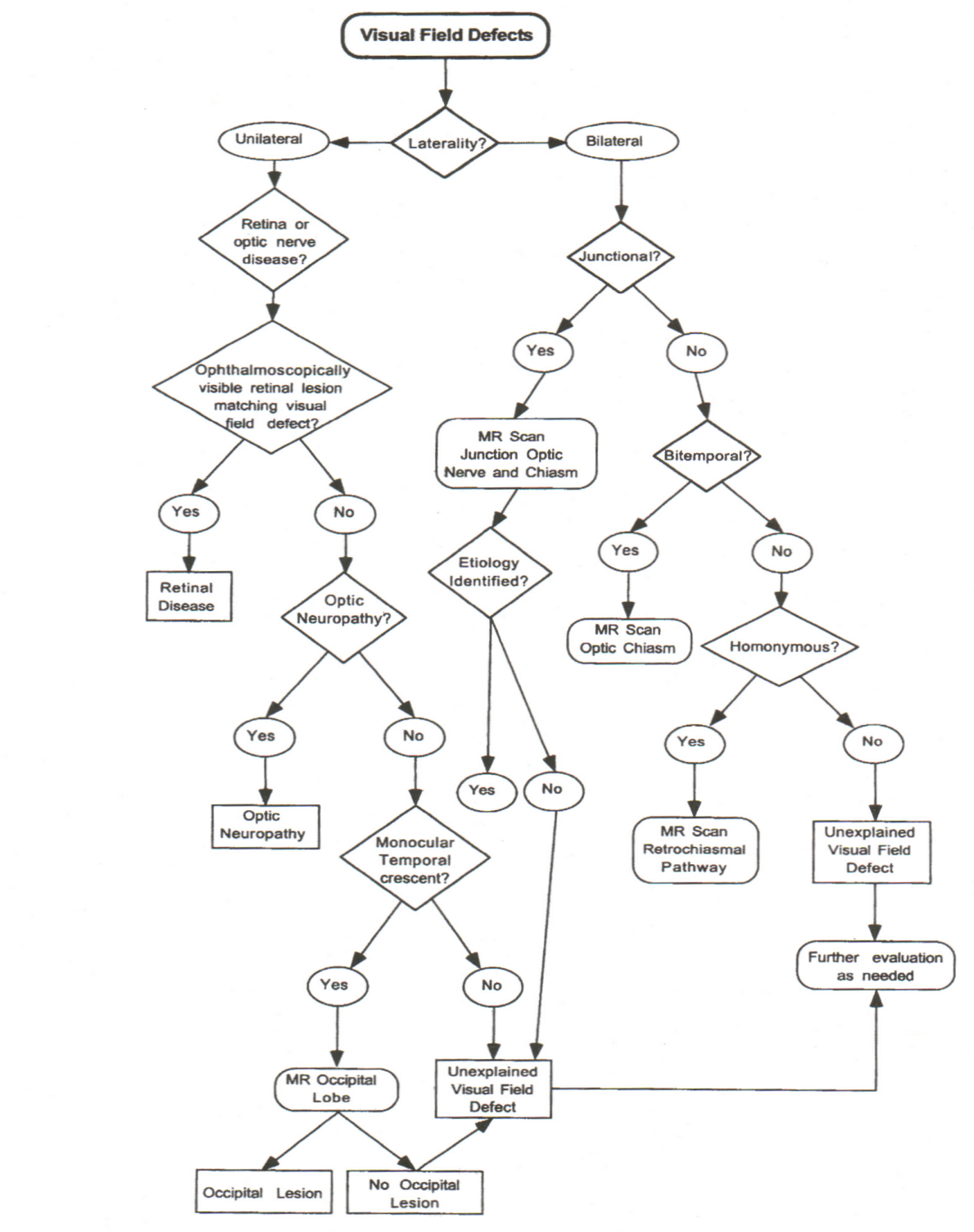
Visual Field Defect Care Path
From: Clinical Pathways in Neuro-ophthalmology 2003
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
3 Visual Fields
Examination of the visual fields helps to localize and identify diseases affecting the visual pathways (▶Fig. 3.1). Visual field testing is useful when evaluating patients complaining of visual loss (especially when the cause of visual loss is not obvious after ophthalmic examination) or patients with neurologic disorders that may affect the intracranial visual pathways (e.g., pituitary tumors, strokes involving the posterior circulation, and traumatic brain injuries).Examination allows localization by correlating the shape of defects to the abnormal portion of the visual pathways. It can be repeated to monitor if the defects are growing or shrinking as a measure of whether the disease process is worsening or improving.
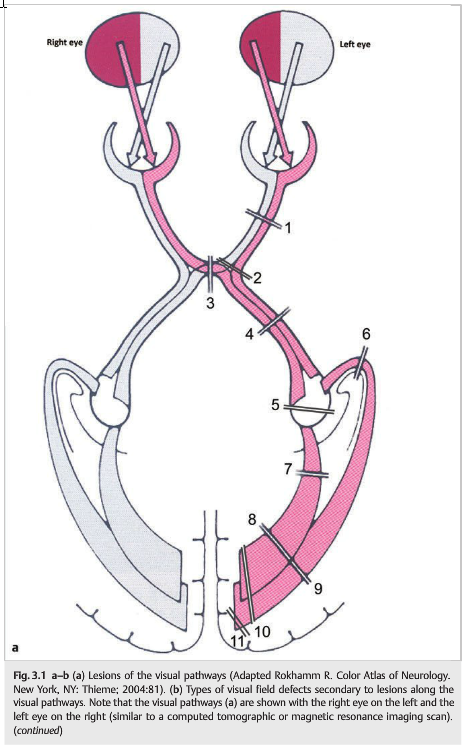
3.1 Visual Pathways
The visual field and retina have an inverted and reversed relationship. Relative to the point of fixation:
● The upper visual field falls on the inferior retina (below the fovea).
● The lower visual field falls on the superior retina (above the fovea).
● The nasal visual field falls on the temporal retina.
● The temporal visual field falls on the nasal retina.
The nasal fibers of the ipsilateral eye (53% of all fibers) cross in the chiasm to join the uncrossed temporal fibers (47% of all fibers) of the contralateral eye. They form the optic tract, which synapses in the lateral geniculate nucleus to form the optic radiations, which terminate in the visual cortex (area 17) of the occipital lobe. Because more fibers in the optic tract come from the opposite eye (crossed fibers), a relative afferent pupillary defect (RAPD) is often observed in the eye contralateral to an optic tract lesion (see discussion later in this chapter).
At the level of the chiasm, the crossing inferonasal fibers travel anteriorly toward the contralateral optic nerve before passing into the optic tract. This is called Wilbrand’s knee and is responsible for the “junctional scotoma” in lesions of the posterior optic nerve. Although the anatomical presence of Wilbrand’s knee is debated, junctional scotomas are observed clinically.
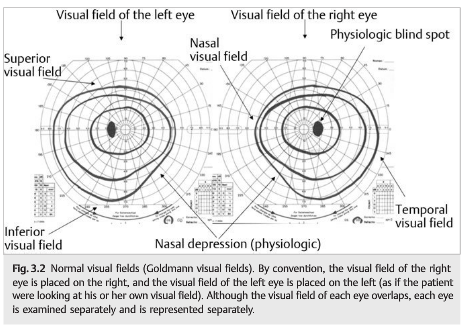
The visual field of each eye overlaps centrally. The normal visual field in each eye is approximately (▶Fig. 3.2).
● 60 degrees superiorly
● 70 to 75 degrees inferiorly
● 60 degrees nasally
● 100 to 110 degrees temporally
The physiologic blind spot corresponds to the optic disc (which has no overlying photoreceptors) and is located approximately 15 degrees temporally in each eye.
3.2 Techniques to Evaluate the Visual Field
Current methods of visual field testing all require the subject to indicate whether the stimulus is seen or not. You cannot reliably test the visual field of an uncooperative or very sick patient. There have been attempts to develop an “objective perimetry” by projecting stimuli on to discrete areas of the retina and using electroretinographic or pupillometric responses as end points, but these methods remain experimental. Visual fields should be tested monocularly given that the overlap in binocular fields may mask visual field defects.
3.2.1 Visual Field Testing at Bedside
Bedside visual field testing is quick and easy but has relatively poor reliability, depending on the patient’s ability to identify and describe the visual field defect.
Face: Ask the patient to look at your nose and tell you if any parts of your face are missing.
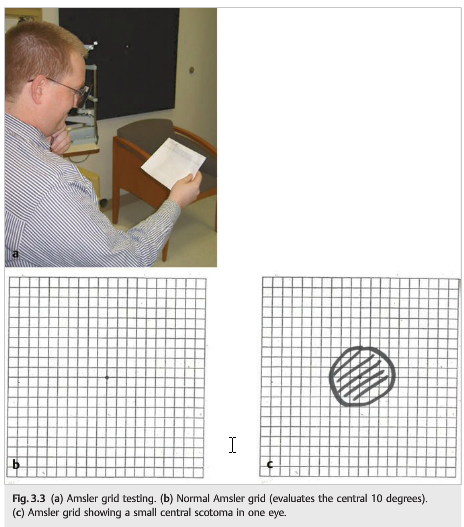
Grid: Present a square grid of lines and ask the patient to fixate on a central point and to draw any area in which the lines disappear (▶Fig. 3.3).
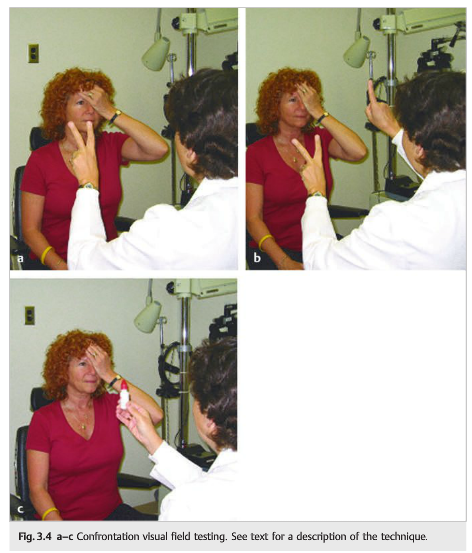
Finger confrontation: This is useful in identifying dense hemianopic or altitudinal defects (▶Fig. 3.4).
The test involves the following steps:
1. Line up the patient across from you.
2. Have the patient cover one eye and stare into the opposite eye on your face with his or her open eye to maintain central fixation.
3. Instruct the patient to count fingers presented within the central 30 degrees (in each of four quadrants around fixation). Special attention should be directed to the horizontal and vertical axes of the visual field to see if there is a change in vision across an axis. The patient should perform the task equally well in all four quadrants.
4. Ask the patient to count fingers in two quadrants simultaneously. If a quadrant of the visual field is consistently ignored, a subtle field defect (or neglect) has been revealed.
5. The far periphery can be assessed by finger wiggle.
6. A consistent difference in color perception (use a red object) across the horizontal or vertical meridian may be the only sign of an altitudinal or hemianopic defect, respectively.
3.2.2 Visual Field Testing in the Office
Tangent Screen
The tangent screen is rarely used and is primarily helpful for evaluating patients suspected of nonorganic constriction of the visual field (▶Fig. 3.5).
The test involves the following steps:
1. The patient sits 1m from a black screen (mounted on a wall) on which there are concentric circles.
2. While the patient is asked to fixate on a central target, a white or colored circular stimulus is slowly moved from the periphery toward the center of the screen until the patient reports seeing the stimulus.
3. By repeating this in various parts of the visual field, an isopter can be plotted and then drawn on the screen with chalk or pins.
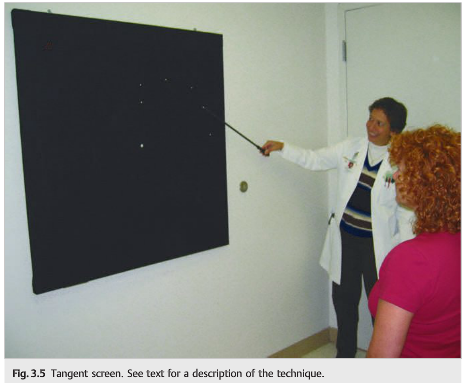
By varying the distance of the patient from the screen, it is possible to differentiate organic from nonorganic constriction of the visual field: in organic patients, the visual field enlarges when the patient is placed farther away from the screen (see Chapter 18).
Goldmann (Kinetic) Perimetry
Goldmann perimetry has the advantage of charting the entire visual field and includes the far temporal periphery (▶Fig. 3.6, ▶Fig. 3.7).
It can quickly establish the pattern of visual field loss in the ill, poorly attentive, or elderly patient who requires continued encouragement to maintain fixation and respond appropriately.
The test involves the following steps:
1. Place the patient’s head on a chin rest on the open side of a white hemispheric bowl.
2. Cover one of the patient’s eyes.
3. Tell the patient to fixate on a central spot.
4. Present stimuli consisting of dots of white light projected one at a time onto the inner surface of the bowl, usually moving from the unseen periphery into the patient’s field of view.
5. Ask the patient to signal detection of the white dot by pressing a buzzer. Note the responses on a chart representing the visual field.
6. Lights of different sizes and brightness allow the drawing of isopters.


The quality of the field is examiner-dependent, and it does not detect subtle changes. Defects are more difficult to quantify than with automated perimetry.
Automated Static Perimetry
Automated perimetry is more sensitive, quantitative, and reproducible, but it is more time consuming and requires good patient cooperation and attention (▶Fig. 3.8).
It is the technique of choice for patients with optic nerve lesions, papilledema, chiasmal compressive lesions, and other progressive visual disorders. Although numerous automated perimetries are available, the Humphrey strategies, in particular, the Swedish Interactive Thresholding Algorithm (SITA) standard and SITA fast programs, are the most commonly used. These tests average about 3minutes (fast) and 6 minutes (standard) per eye.
The test involves the following steps:
1. Place the patient’s head on a chin rest in front of a computer screen.
2. Cover one of the patient’s eyes.
3. Tell the patient to fixate on a central spot.
4. Present stimuli consisting of dots of white light projected one at a time onto the screen, randomly presented (not moving).
5. Ask the patient to signal detection of the white dot by pressing a buzzer.
6. The stimulus size is kept the same, but the brightness varies.
7. Only the central 10, 24, or 30 degrees is usually tested.

3.3 Interpretation of a Visual Field Defect
3.3.1 Understanding a Humphrey Visual Field Printout
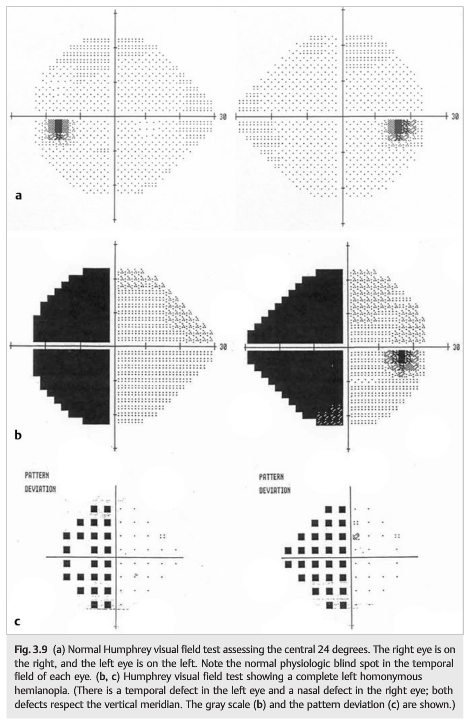
Humphrey perimetry uses computerized programs to randomly test points in the patient’s central visual field with a standard stimulus size but varying stimulus intensities (▶Fig. 3.9).
It uses a threshold strategy, in which the stimulus intensity varies and is presented multiple times at each location so that the level of detection of the dimmest stimulus is determined. This is then reported on a computerized printout in various ways, some numerical, others pictorial.
3.3.2 Assessing the Quality of the Visual Field
The ability of the patient to perform the test can be evaluated by measurements of reliability reported on the printout. In the example provided in ▶Fig. 3.10, the left eye was tested (as indicated by the word left in the upper right corner). Reliability measurements are reported in the upper left corner and include the number of fixation losses (2/13), false-positive errors (0%), and false-negative errors (3%) during the test. A large number of fixation losses (>33% of false-positive or false-negative responses) indicates an unreliable test.
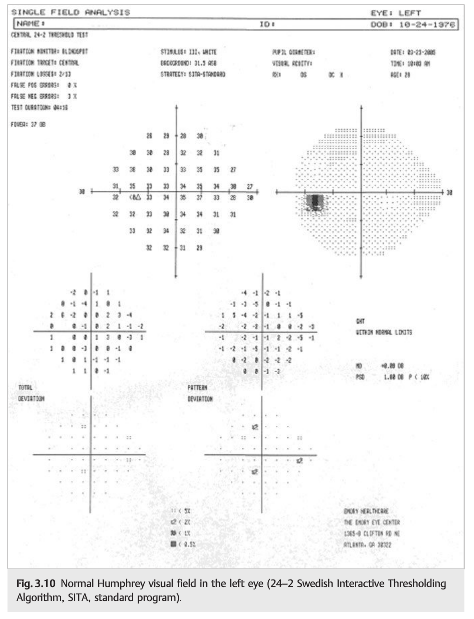
3.3.3 Interpreting the Visual Field Test
The numeric grid just to the right of the measurements of reliability is a presentation of the threshold level in decibels for all points checked in the patient’s visual field. A recorded number of 0 indicates that the patient could not detect even the brightest stimulus at that point. The higher the number, the better the vision at that point in the field. These numbers are then converted to a gray scale representation of the field (upper right, ▶Fig. 3.10), which provides a gross picture of the size and severity of the field defects present. A comparative scale on the bottom relates the degree of grayness on the gray scale to the change in decibel levels from the numeric grid. The number scale labeled “Total Deviation” in ▶Fig. 3.10 indicates the amount each point deviates from the age-adjusted normal values. In this case, the more negative a number, the more abnormal that point. The number scale to the right in ▶Fig. 3.10 labeled “Pattern Deviation” highlights focal abnormalities in the visual field, helping to emphasize the pattern of visual field loss.
Pearls
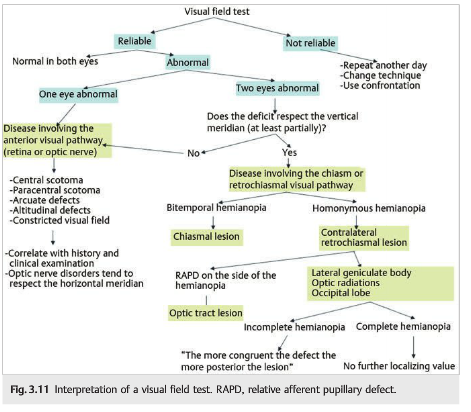
In interpreting a visual field test, you need to ask the following questions (▶Fig. 3.11):
1. Is the test reliable (as indicated by the technician for Goldmann visual fields and by the reliability parameters for automated perimetry)?
2. Is the test normal or not?
3. Does the visual field defect involve one eye or two eyes?
4. If binocular, does the defect respect the vertical meridian?
5. If it respects the vertical meridian, is the defect bitemporal (temporal side of the vertical meridian in each eye) or homonymous (on the same side of the vertical meridian in each eye)?
6. If it is homonymous, is the defect complete or incomplete?
7. If it is homonymous and incomplete, is the defect congruent (same defect shape and size in each eye)?
3.4 Topographic Diagnosis of Visual Field Defects
Characterization of the visual field defect often allows precise localization of the lesion along the visual pathways. Once the lesion is localized anatomically, a directed workup looks for an etiology.
3.4.1 Anterior Visual Pathways
Retina
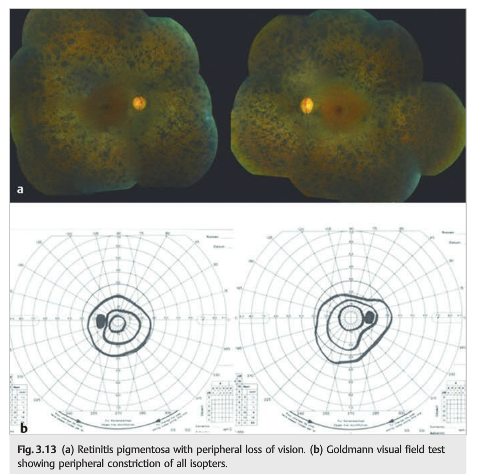
Macular lesions produce central or paracentral defects, whereas most degenerative retinopathies, such as retinitis pigmentosa, produce progressive constriction of the peripheral and midperipheral visual field (▶Fig. 3.12 and ▶Fig. 3.13).

Optic Nerve
Optic neuropathies typically produce nerve fiber bundle defects within the central 30 degrees of the visual field. Depending on the etiology of the optic neuropathy, arcuate defects, altitudinal defects, and central, paracentral, or centrocecal scotomas are observed (▶Fig. 3.14, ▶Fig. 3.15, ▶Fig. 3.16).



Chiasm
The nasal retinal fibers of each eye cross in the chiasm to the contralateral optic tracts, and the temporal fibers remain uncrossed. Thus a chiasmal lesion will cause a bitemporal hemianopia due to interruption of decussating nasal fibers (▶Fig. 3.17 and ▶Fig. 3.18).


3.4.2 Retrochiasmal Visual Pathways
Retrochiasmal lesions involving the visual pathways produce a contralateral homonymous hemianopia.
Complete homonymous hemianopias may occur with any lesion of the retrochiasmal visual pathways and do not allow precise localization of the lesion along the retrochiasmal visual pathways. Incomplete homonymous hemianopias may help localize the lesion based on their congruity:
● Hemianopia is incongruent when visual field defects are different in each eye.
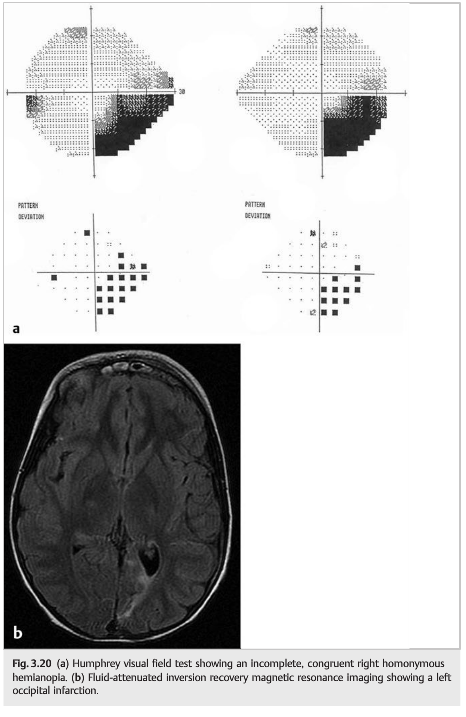
● Hemianopia is congruent when visual field defects are identical in each eye. The rule of congruency states that the more congruent the homonymous hemianopia, the more posterior the lesion. (This rule does not apply to optic tract lesions that are suspected when the homonymous hemianopia is associated with a RAPD on the side of the hemianopia and bilateral optic nerve pallor). ▶Fig. 3.19, ▶Fig. 3.20, and ▶Fig. 3.21 show different homonymous hemianopias.
Optic Tract
Lesions of the optic tract cause a contralateral homonymous hemianopia, which may or may not be congruent.
Optic tract fibers are the axons of the ganglion cells originating in the inner layers of the retina. These axons are destined for the lateral geniculate nucleus, where they synapse with neurons whose axons then form the optic radiations. Therefore, chronic optic tract lesions will cause optic atrophy, often in a characteristic pattern.
Lesions of the optic tract (left optic tract lesion in the example in ▶Fig. 3.22) produce atrophy of three groups of retinal ganglion cell fibers:
1. Nasal half of the macula of the right eye ([1–red] in ▶Fig. 3.22d)
2. Nasal retina of the right eye ([2–red]) in ▶Fig. 3.22d)
3. Temporal retina in the left eye ([3–green] in ▶Fig. 3.22d)
Lesion groups 1 and 2 result in a bowtie pattern of optic atrophy (▶Fig. 3.22b) of the right optic nerve. Lesion group 3 results in mostly temporal atrophy of the left optic nerve (▶Fig. 3.22b). A RAPD is often observed in the eye contralateral to the optic tract lesion. This is because more fibers in the optic tract come from the opposite eye, having crossed in the chiasm. This greater contribution from the opposite eye is because the nasal retina is bigger than the temporal retina (the temporal visual field is bigger than the nasal visual field in each eye). The resultant RAPD will be in the eye that has contributed the most fibers to the damaged optic tract (i.e., the eye opposite the lesion, on the same side as the homonymous hemianopia).


Pearls
A left optic tract syndrome includes the following:
● Right homonymous hemianopia
● Right RAPD
● Bowtie atrophy of the right optic nerve
● Mostly temporal pallor of the left optic nerve
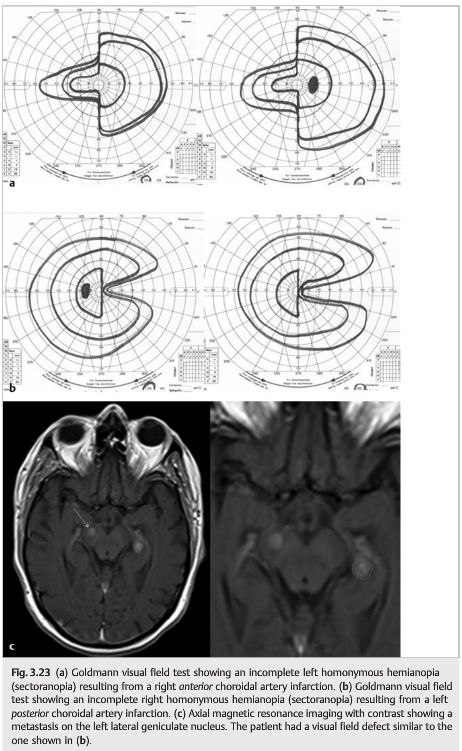
Lateral Geniculate Nucleus
Lesions of the lateral geniculate nucleus typically cause a contralateral homonymous hemianopia. Two patterns of visual field loss occur when the lesion is secondary to an ischemic lesion in the territory of the choroidal arteries (anterior or posterior) (▶Fig. 3.23).
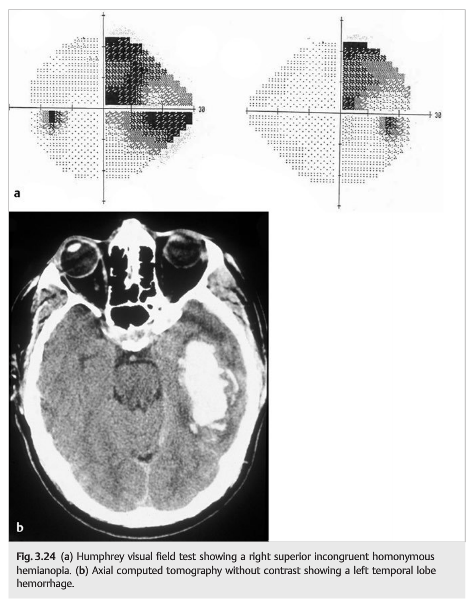
Optic Radiations
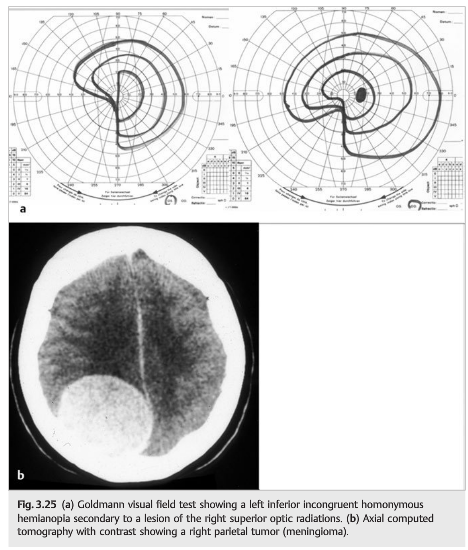
Lesions of the optic radiations typically produce a contralateral homonymous hemianopia, worse superiorly when the lesion is in the temporal lobe and worse inferiorly when the lesion is in the parietal lobe. Postsynaptic fibers from the lateral geniculate nucleus form the optic radiations, which separate into the inferior fibers (temporal lobe) and the superior fibers (parietal lobe) as they progress posteriorly toward the occipital cortex (▶Fig. 3.24). Lesions of the parietal lobe often impair optokinetic nystagmus (see ▶Fig. 1.27) when stimuli are moved in the direction of the damaged parietal lobe (▶Fig. 3.25).
Occipital Lobe: Unilateral
Lesions of the occipital lobe produce a contralateral homonymous hemianopia, which is most often congruent. Most isolated congruent homonymous hemianopias are due to an occipital infarction in the territory of the posterior cerebral artery (PCA).
The tip of the occipital lobe, where the macular or central homonymous hemifields are represented, often has a dual blood supply from terminal branches of the PCA and of the middle cerebral artery (MCA). Depending on anatomical variations of the blood supply and of the circle of Willis, the tip of the occipital lobe is often a watershed area ▶ Fig. 3.26).

Occlusion of the PCA often results in sparing of the tip of the occipital lobe, thereby sparing the macular representation, which is vascularized by terminal branches of the MCA (▶Fig. 3.27).

An embolic infarction of either a distal MCA or PCA branch can result in exclusive ischemia of the tip of the occipital lobe, thereby producing a small homonymous scotomatous defect if there is inadequate collateral circulation (▶Fig. 3.28).
Occipital Lobe: Sparing the Temporal Crescent
When we fixate with both eyes, there is superimposition of the central 60 degrees of visual fields in both eyes. There remains in each eye a temporal crescent of visual field for which there are no corresponding points in the other eye. The representation of this most peripheral 20 to 30 degrees is located in the anterior most portion of the contralateral occipital cortex. Lesions of the occipital lobe sparing this anterior most portion of the occipital cortex will spare the temporal crescent (▶Fig. 3.29).
Occipital Lobe: Bilateral
Bilateral occipital lobe lesions will produce bilateral homonymous hemianopias, which may be asymmetric (▶Fig. 3.30). In addition to the visual field defects, there may be decreased visual acuity, which is always the same in both eyes (▶Fig. 3.31).

Pearls
When bilateral lesions of the retrochiasmal visual pathways produce a decrease in visual acuity, the degree of visual acuity loss is always symmetric in both eyes, unless there are other, more anterior, reasons for a decrease in visual acuity (e.g., asymmetric refractive errors, cataracts, or a superimposed asymmetric or unilateral retinopathy or optic neuropathy).
The information below is from: The temporal crescent syndrome. Ali K. Pract Neurol 2015;15:53–55
ABSTRACT
Retro-chiasmal lesions almost always give rise to homonymous field defects with only one exception. The nasal visual field extends to 60% of the horizon, whereas the temporal field extends to a further 30°–40° beyond that; this part of the visual field is represented on the contralateral anterior parieto-occipital sulcus. A lesion in this area will give rise to monocular visual field defect affecting the contralateral eye. This is called the temporal crescent or the half moon syndrome. In this case report, a woman presented with seizures secondary to haemorrhagic infarction of the anterior part of the parieto-occipital sulcus. She later presented with right-sided visual disturbance; her examination confirmed temporal crescent syndrome. I explain the pathophysiology of this rare neurological syndrome in this report.
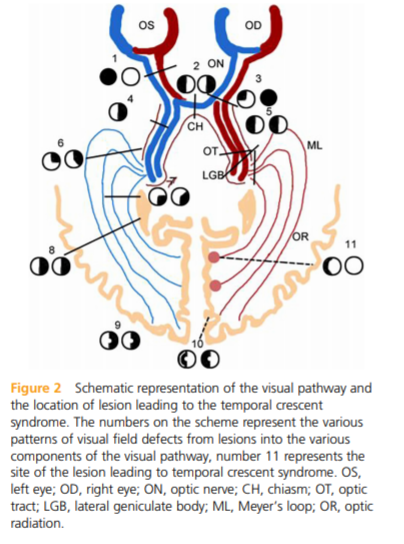
Learning points
▸ Retro-chiasmal lesions normally cause homonymous visual field defects; the only exception is the ‘temporal crescent’ or ‘half moon syndrome’, caused by a lesion in the anterior part of the contralateral parieto-occipital sulcus.
▸ The most nasal retinal fibers have unpaired cortical representation, which is situated in the most anterior part of the contralateral parieto-occipital sulcus.
References:
1. Clinical Pathways in Neuro-ophthalmology. Stacy Smith, Andrew Lee, Paul Brazis. 2003. Thieme
2. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
2. The temporal crescent syndrome. Ali K. Pract Neurol 2015;15:53–55
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.