Questions:
11. What causes autofluorescence in the fundus?
12. What are the abnormal states of lipofuscin?
13. Do optic nerve drusen cause hyperautofluorescence or hypoautofluorescence?
14. Fluorescein angiography can help differentiate macular from optic nerve related visual loss. True or False?
15. Demonstration of retinal small vessel vasculopathy such as vasculitis is best done with retinal fluorescein angiography. True or False?
16. How is ultrasound helpful in assessing papilledema/pseudopapilledema?
17. What are 7 indications for B-scan echography?
____________________________________________________
Questions with answers:
11. What causes autofluorescence in the fundus?
Autofluorescence is caused by the presence of lipofuscin, an aging pigment fluorophore produced by the outer segments of the photoreceptors and stored at the level of the retinal pigment epithelium.
12. What are the abnormal states of lipofuscin?
Two abnormal states of lipofuscin exist, hyperautofluorescence and hypoautofluorescence; both are associated with various retinal disorders.
13. Do optic nerve drusen cause hyperautofluorescence or hypoautofluorescence?
Optic nerve head drusen are usually hyperautofluorescent.
14. Fluorescein angiography can help differentiate macular from optic nerve related visual loss. True or False?
True – FA can help differentiate macular from optic nerve–related visual loss by 1. showing macular changes that are not always easily visible on funduscopic examination, or 2. showing a normal macula with leakage from the optic disk.
15. Demonstration of retinal small vessel vasculopathy such as vasculitis is best done with retinal fluorescein angiography. True or False?
True – The abnormal vessels leak on fluorescein angiography and vascular abnormalities that are missed on fundus examination may be seen on fluorescein angiography.
16. How is ultrasound helpful in assessing papilledema/pseudopapilledema?
Measurement of the optic nerve diameter 3 mm posterior to the sclera by has demonstrated to enable US and MRI provide measurements of optic nerve diameter that are well-correlated and sensitive markers for increased ICP.2
Ultrasound may confirm pseudopapilledema by demonstrating the typical findings of optic nerve head drusen, including buried drusen.
17. What are 7 indications for B-scan echography?
1. Differentiating pseudopapilledema from papilledema
2. Trauma with a poor view of the fundus to demonstrate vitreous hemorrhage or retinal detachment
3. Identification of an intraocular foreign body
4. Analysis of intraocular and orbital pole tumors
5. Examination of the extraocular muscles
6. Examination of the superior ophthalmic vein when a carotid-cavernous fistula is suspected
7. Posterior scleritis (T-sign)
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
4.2 Fundus Autofluorescence
Fundus autofluorescence (FAF) imaging is helpful in diagnosing retinal conditions at an early stage by showing abnormalities that are often invisible to standard fundus photography and ophthalmoscopy (▶Fig. 4.5).
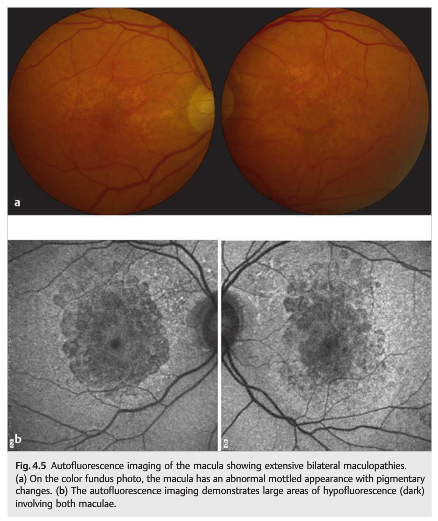
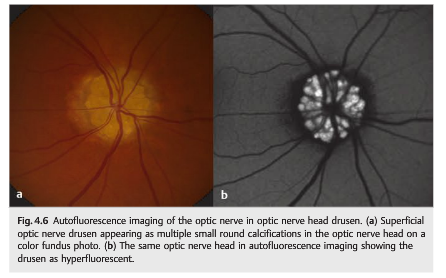
Autofluorescence is caused by the presence of lipofuscin, an aging pigment fluorophore produced by the outer segments of the photoreceptors and stored at the level of the retinal pigment epithelium. Two abnormal states of lipofuscin exist, hyperautofluorescence and hypoautofluorescence (▶Fig. 4.5b); both are associated with various retinal disorders. Optic nerve head drusen are also usually hyperautofluorescent (▶Fig. 4.6).
4.3 Retinal Fluorescein Angiography
Intravenous (IV) fluorescein angiography is a photographic method of angiography that does not rely on radiation. After IV injection of fluorescein solution (in an arm vein),rapid-sequence retinal photography is performed by using a camera with spectrally appropriate excitation and filters (the fluorescein absorbs blue light and becomes fluorescent, which can be captured on photographs).
Fluorescein angiography is helpful in studying the vascular filling patterns of the choroidal, retinal, and optic nerve head arteries and veins. It can also help differentiate macular from optic nerve–related visual loss by showing macular changes that are not always easily visible on funduscopic examination. However, imaging of the macula with optical coherence tomography has now replaced fluorescein angiography for most of these cases.
The test requires the cooperation of the patient, who needs to be able to sit up and fixate. It also requires relatively clear ocular media.
Fluorescein angiography is usually well tolerated, although side effects include nausea, vomiting, and vasovagal responses. True allergic reactions are rare. The fluorescein is excreted in the urine (which becomes yellow and fluorescent) within 24 to 36 hours.
The technique for fluorescein angiography is as follows. Color photos and red-free photos are taken prior to the injection of fluorescein. Once the fluorescein is injected, multiple retinal photos are taken on the same eye (chosen by the clinician) to study the choroidal and retinal vascular filling dynamic. A time (since the injection) is noted on each photo (▶Fig. 4.7).

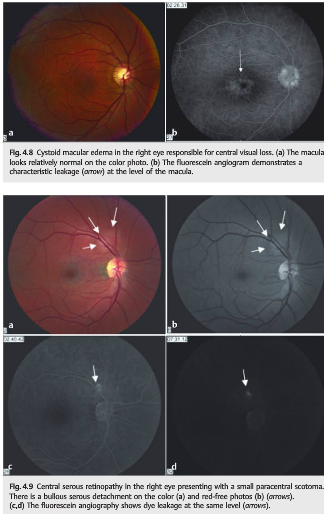
Delay in the choroidal filling, as well as delay or asymmetry in the retinal vascular filling, is indicative of vascular disease. Photos are then taken of both eyes depending on the reason for the test. Abnormal fluorescence of the retina (indicating staining, pooling, or leakage of the fluorescein or blockage of the fluorescence) is indicative of retinal or choroidal disorders. Late photos may show leakage of the vessels (as in vasculitis) or of the optic nerve (as in optic nerve edema) (▶Fig. 4.8and ▶Fig. 4.9).
Demonstration of retinal small vessel vasculopathy such as vasculitis is best done with retinal fluorescein angiography. The abnormal vessels leak and vascular abnormalities may be missed on fundus examination (▶Fig. 4.10).
Fluorescein angiography is also very helpful for the diagnosis of giant cell arteritis. Photographs should be taken of both eyes with transit (early images after injection of IV fluorescein) on the most affected eye (▶Fig. 4.11).


4.4 Optical Coherence Tomography
Optical coherence tomography (OCT) is routinely performed in ophthalmology. It is a noninvasive transpupillary ophthalmic imaging technology that can image retinal and optic nerve structures in vivo with a resolution of 4µm. Cross-sectional images of the retina, the optic nerve, and peripapillary areas are produced using the optical backscattering of light similar to what is obtained with a B-scan ultrasound (OCT uses low-coherence near-infrared light). The anatomical layers within the retina can be differentiated, and retinal thickness can be measured (▶Fig. 4.12).

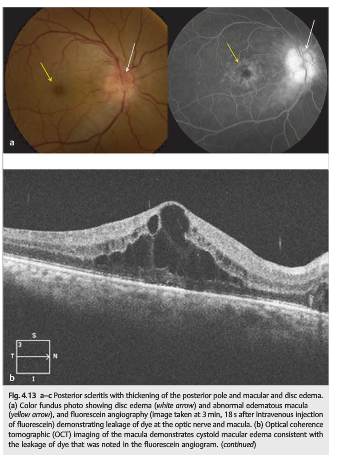
OCT is particularly useful for macular diseases (▶Fig. 4.13); however, it requires a patient’s ability to fixate and relatively clear ocular media. The quality is often better when the pupils are pharmacologically dilated. OCT is very useful in demonstrating anatomical changes in the macular, such as edema (▶Fig. 4.13), holes, cysts, macular traction, and an epiretinal membrane.
Additionally, individual retinal layers can be analyzed and the retinal nerve fiber layer thickness and macular volume can be measured with OCT (▶Fig. 4.14).
This is important because peripapillary nerve fiber thickness and macular volume are decreased in glaucoma and other diseases of the optic nerve, such as optic neuritis. They are used to monitor disease activity in numerous optic neuropathies.

4.5 Ocular/Orbital Echography
Echography, or ultrasound, is a technique that uses high-frequency sound waves to image tissue. Tissue characteristics such as increased cell density and reflective surfaces determine the specific echographic pattern.
Ocular and orbital echography is performed by applying a probe directly to the eye (on the eyelid or directly on the corneal surface). The amount of energy returned to and detected by the probe determines the height (A scan) or intensity (B scan) of the resultant image.
A-scan echography is usually not used in neuro-ophthalmology (it allows measurement of ocular axial length such as for calculation of intraocular lens power before cataract surgery, as well as analysis of choroidal tumors).
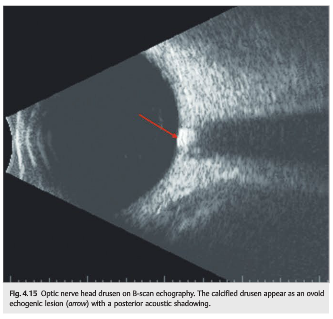
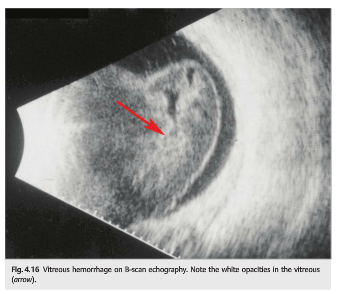
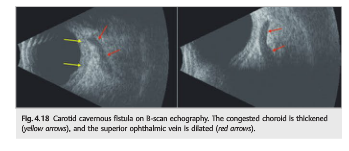
B-scan echography shows a two-dimensional image representing a “slice” through the globe. It is therefore particularly useful in examining the posterior pole in patients with vitreous opacities in whom the retina cannot be visualized, or to visualize calcified optic nerve drusen, and to evaluate a choroidal mass. It can also evaluate the anterior orbit and is used to measure the extraocular muscles in suspected thyroid eye disease and the superior ophthalmic vein when a carotid cavernous fistula is suspected.
Indications for B-scan echography in neuro-ophthalmology include the following:
● Optic nerve head drusen (may not be seen on fundus examination when buried)(▶Fig. 4.15)
● Trauma with poor view of the fundus to demonstrate vitreous hemorrhage(▶Fig. 4.16) or retinal detachment (▶Fig. 4.17)
● Identification of an intraocular foreign bod ● Analysis of posterior pole tumors
● Examination of the extraocular muscles when thyroid eye disease is suspected
● Examination of the superior ophthalmic vein when a carotid-cavernous fistula is suspected (▶Fig. 4.18)
● Posterior scleritis (T-sign) (see ▶Fig. 4.13c)

References:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
2. Comparison of Ocular Ultrasonography and Magnetic Resonance Imaging for Detection of Increased Intracranial Pressure. Patterson DF, Ho M-L, Leavitt JA, Smischney NJ, Hocker SE, Wijdicks EF, Hodge DO, John JingChen JJ-W Front Neurol. 2018; 9: 278.
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.