Questions:
1. The visual evoked response is not accurate if the patient fails to cooperate. True or False?
2. The visual evoked response is primarily a function of central visual function. True or False?
3. Visual evoked responses are most useful in evaluating the integrity of the visual pathway in infants and inarticulate adults. True or False?
4. In optic neuropathy, the ERG should be normal. True or False?
5. Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss. True or False?
6. The ERG is invariably severely depressed by the time patients complain of visual loss due to retinal disease. True or False?
7. Can a patient substantially alter the full-field ERG voluntarily?
8. Can a patient substantially alter the multifocal ERG voluntarily?
9. Multifocal ERGs are extremely helpful in detecting occult focal retinal abnormalities within the macula. True or False?
10. The multifocal ERG simultaneously records locations within the central 30 degrees. True or False?
____________________________________________________
Questions with answers:
1. The VER is not accurate if the patient fails to cooperate. True or False?
True – Abnormal responses may occur if the patient does not look at the screen, does not focus on the screen, moves the tested eye, or is tired. Appropriate refraction is necessary.
2. The VER is primarily a function of central visual function. True or False?
True – The visual evoked response reflects the integrity of the afferent visual pathway (damage anywhere from the retina to the occipital cortex may alter the signal). It is primarily a function of central visual function because such a large region of the occipital cortex near the recording electrodes is devoted to macular projections.
3. VERs are most useful in evaluating the integrity of the visual pathway in infants and inarticulate adults. True or False?
True – VERs are most useful in evaluating the integrity of the visual pathway in infants and inarticulate adults. A preserved flash or pattern response confirms intact pathways, whereas an abnormal flash response indicates gross impairment. An abnormal pattern response is less useful: it may indicate damage, or it may be falsely abnormal.
4. In optic neuropathy the ERG should be normal. True or False?
TRUE
5. Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss. True or False?
TRUE
6. The ERG is invariably severely depressed by the time patients complain of visual loss due to retinal disease. True or False?
True – The ERG is invariably severely depressed by the time patients complain of visual loss.
7. Can a patient substantially alter the full-field ERG voluntarily?
No, although poorly cooperative patients can make interpretation of the full-field ERG more difficult. There can be background noise due to frequent blinking and squeezing, but the responses cannot be substantially altered voluntarily unlike visual evoked responses.
8. Can a patient substantially alter the multifocal ERG voluntarily?
Yes, uncooperative patients can alter the responses on a multifocal ERG by not fixating accurately.
9. Multifocal ERGs are extremely helpful in detecting occult focal retinal abnormalities within the macula. True or False?
TRUE
10. The multifocal ERG simultaneously records locations within the central 30 degrees. True or False
True – The multifocal ERG simultaneously records ERG signals from up to 250 focal retinal locations within the central 30 degrees.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
4 Ancillary Testing Commonly Used in Neuro-ophthalmology
In most cases, decisions regarding lesion localization and presumed etiology are determined based on the clinical history and examination. Ancillary testing should be obtained only to confirm or to document a clinical impression, not to “go fishing” for an answer.
Knowing what to look for before ordering ancillary testing will allow you to recommend the appropriate test and interpret that test correctly. For example, brain imaging obtained for the evaluation of a third nerve palsy may demonstrate a Chiari malformation. In this case, the Chiari malformation should be considered an incidental finding that is asymptomatic and that does not need to be treated or investigated further.
4.1 Electrophysiologic Testing
Electrophysiologic testing can help differentiate retinal from optic nerve disease in selected cases. It is also helpful in documenting occult abnormalities of the optic nerve or retinal function.
4.1.1 Visual Evoked Responses (or Visual Evoked Potentials)
Visual evoked responses (or visual evoked potentials) are measurements of the electrical signal recorded at the scalp over the occipital cortex in response to visual stimuli. In the test, the patient is asked to look at a TV screen on which various stimuli are provided; electrodes placed on the scalp over the occipital cortex record the responses. Each eye is tested separately.
This test is not accurate if the patient does not cooperate. Abnormal responses may occur if the patient does not look at the screen, does not focus on the screen, moves the tested eye, or is tired. Appropriate refraction is necessary.
The visual evoked response reflects the integrity of the afferent visual pathway (damage anywhere from the retina to the occipital cortex may alter the signal). It is primarily a function of central visual function because such a large region of the occipital cortex near the recording electrodes is devoted to macular projections.
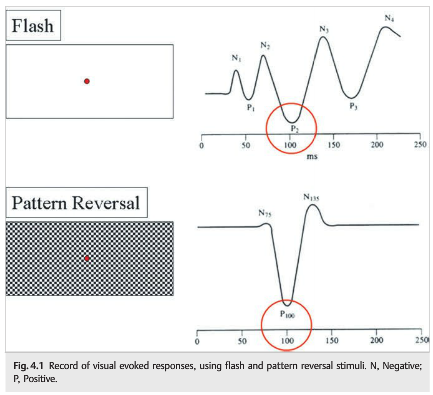
Two techniques are used to record visual evoked responses: pattern stimulus, which provides a quantifiable and reliable waveform but may be absent in patients with poor vision, and flash stimulus, which is useful for patients with very poor vision in whom the pattern stimulus response is absent. The recorded responses for each eye are then compared (▶Fig. 4.2), with the focus on the amplitude and peak latency of the wave-form (P100). Classically, the P100 waveform is delayed in patients with demyelinating optic neuritis.
In most clinical situations, the visual evoked responses are of limited usefulness and are not necessary to make the diagnosis of optic neuropathy.
Visual evoked responses are most useful in evaluating the integrity of the visual pathway in infants and inarticulate adults. A preserved flash or pattern response confirms intact pathways, whereas an abnormal flash response indicates gross impairment (▶Fig. 4.2). An abnormal pattern response is less useful: it may indicate damage, or it may be falsely abnormal.
Visual evoked responses are also useful in confirming intact visual pathways in patients with markedly abnormal subjective visual responses of suspected nonorganic origin. A response with an intact pattern not only confirms intact visual pathways but also provides an estimate of visual acuity when stimuli of various sizes are used. A response with an abnormal or absent pattern does not confirm organic disease because voluntary inattention or defocusing can markedly alter the pattern waveform.
4.1.2 Electroretinogram
Electroretinogram
The electroretinogram (ERG) is a measurement of electrical activity of the retina in response to light stimulus. It is measured at the corneal surface by electrodes embedded in a corneal contact lens worn for testing. The ERG is normal in optic neuropathies.

Full-Field Electroretinogram
A full-field ERG is generated by stimulating the entire retina with a flash light source under varying conditions of retinal adaptation to dark and light (▶Fig. 4.3).
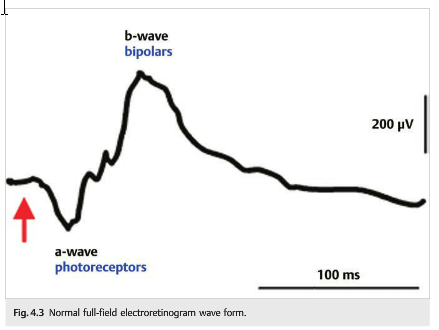
Major components of the electrical waveform generated and measured include the following:
● A wave (negative): primarily derived from the photoreceptor layer (outer retina)
● B wave (positive): derived from the inner retina (Müller and bipolar cells)
● Two other waveforms that are sometimes recorded are the c-wave originating in the pigment epithelium and the d-wave indicating activity of the OFF bipolar cells.
Rod and cone photoreceptors can be separated by varying stimuli and the state of retinal adaptation during testing.
Full-field ERG is useful in detecting diffuse retinal disease in the setting of generalized or peripheral vision loss. Disorders such as retinitis pigmentosa, cone-rod dystrophy, toxic retinopathies, and retinal paraneoplastic syndromes may present with variably severe visual loss and minimally visible retinal abnormalities. The ERG is invariably severely depressed by the time patients complain of visual loss, making full-field ERG testing very useful. Although poorly cooperative patients can make interpretation of the full-field ERG more difficult (there can be background noise due to frequent blinking and squeezing), the responses cannot be substantially altered voluntarily (unlike visual evoked
Because the full-field ERG measures only a mass response of the entire retina, it may be normal in minor or localized retinal disease, particularly maculopathies, even with severe visual acuity loss.
4.2 Multifocal Electroretinogram
Multifocal ERG simultaneously records ERG signals from up to 250 focal retinal locations within the central 30 degrees. The individual responses are mapped topographically (▶Fig. 4.4).
This technique is extremely helpful in detecting occult focal retinal abnormalities within the macula. Unlike full-field ERG, however, uncooperative patients can alter the responses on a multifocal ERG by not fixating accurately.

Because electrophysiologic testing often provides diagnostic clues as to the etiology of the unexplained visual loss, it should be part of the neuro-ophthalmologic examination in selected patients.
4.2 Fundus Autofluorescence
Fundus autofluorescence (FAF) imaging is helpful in diagnosing retinal conditions at an early stage by showing abnormalities that are often invisible to standard fundus photography and ophthalmoscopy (▶Fig. 4.5).
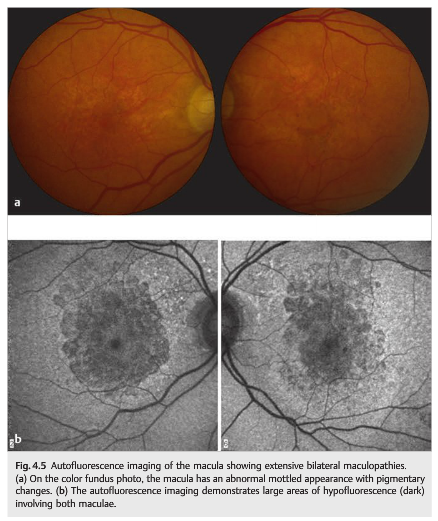
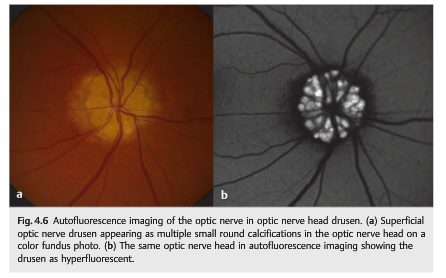
Autofluorescence is caused by the presence of lipofuscin, an aging pigment fluorophore produced by the outer segments of the photoreceptors and stored at the level of the retinal pigment epithelium. Two abnormal states of lipofuscin exist, hyperautofluorescence and hypoautofluorescence (▶Fig. 4.5b); both are associated with various retinal disorders. Optic nerve head drusen are also usually hyperautofluorescent (▶Fig. 4.6).
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.