18. What findings are likely to be present with ethambutol toxicity?
19. On MRI T1-weighted non-contrast images are each of the following structures hyperintense, or hypointense: fat, vitreous, CSF, subacute blood?
20. To improve the evaluation of orbital structures, what MRI techniques should be requested?
21. On MRI T2-weighted non-contrast images are the following structures hyperintense, or hypointense: fat, vitreous, CSF?
22. What special MRI sequence allows transformation of the bright CSF signal into a black signal while maintaining the other characteristics of a T2-weighted image?
23. What MRI technique is ideal for detecting acute cerebral ischemia?
24. What 5 techniques may be helpful in detecting optic nerve head drusen?
25. What MRI technique allows better visualization of blood products, such as hemosiderin?
26. What is Isodense on CT?
27. What is hypodense on CT?
28. What is hyperdense on CT?
29. What enhances with contrast on CT?
30. What are 7 good indications for CT?
31. What are 7 good indications for MRI?
_______________________________________________
Questions with answers:
18. What findings are likely to be present with ethambutol toxicity?
Ethambutol toxicity can cause bilateral optic neuropathy. The findings include: decreased acuity, reduced color vision, bilateral central or cecocentral scotomas, rarely bitemporal scotomas, optic discs may be normal initially or slight hyperemic, later there is disk pallor. OCT has not been demonstrated to be useful in detecting early ethambutol toxicity. Age, hypertension and renal diseases increase the risk of toxicity.
19. On MRI T1-weighted non-contrast images are each of the following structures hyperintense, or hypointense: fat, vitreous, CSF, subacute blood?
Hyperintense: Fat and subacute blood.
Hypointense: Vitreous and CSF.
On T1-weighted images, brain gray matter is gray, and brain white matter is lighter.
Most cerebral parenchymal lesions appear dark (hypointense), unless gadolinium contrast is given; in that case, and if there is a breakdown in the blood-brain barrier, they may appear white (hyperintense).
20. To improve the evaluation of orbital structures, what MRI techniques should be requested?
Orbital MRI should include the following:
● Thin cuts
● Axial T1 sequence
● Axial T1 sequence with fat suppression
● Axial T1 sequence with fat suppression after injection of contrast
● Coronal T1 sequence with fat suppression
● Coronal T1 sequence with fat suppression after injection of contrast
21. On MRI T2-weighted non-contrast images are the following structures hyperintense, or hypointense: fat, vitreous, CSF?
Hyperintense: Vitreous and CSF.
Hypointense: Fat.
On T2-weighted images, brain gray matter is lighter than brain white matter.
T2-weighted images are ideal for screening for brain parenchymal abnormalities.
Additionally, most cerebral parenchymal lesions appear bright (hyperintense), especially inflammatory or ischemic lesions.
22. What special MRI sequence allows transformation of the bright CSF signal into a black signal while maintaining the other characteristics of a T2-weighted image?
Fluid-attenuated inversion recovery (FLAIR) images.
Because the ventricles are filled with CSF, a regular T2 sequence shows the ventricles, and the subarachnoid space as very bright and does not allow for good evaluation of periventricular lesions, such as the white matter lesions from multiple sclerosis. A specific sequence called fluid-attenuated inversion recovery (FLAIR) allows transformation of the bright CSF signal into a black signal, while maintaining the other characteristics of a T2-weighted image. FLAIR images are therefore “black CSF” T2-weighted images.
23. What MRI technique is ideal for detecting acute cerebral ischemia?
Diffusion weighted imaging (DFI). An increased diffusion-weighted imaging signal in ischemic brain tissue is observed within a few minutes after arterial occlusion and progresses through a stereotypic sequence of apparent diffusion coefficient (ADC) reduction, followed by subsequent increase, pseudo-normalization and, finally, permanent elevation. Reported sensitivity ranges from 88-100% and specificity ranges from 86-100%.
24. What 5 techniques may be helpful in detecting optic nerve head drusen?
1. Ophthalmoscopy
2. Auto-fluorescent disk photos – drusen autofluoresce
3. B scan ultrasound – optic nerve head contains highly reflective area; even on decreasing the sensitivity of the display, calcified drusen maintains high signal intensity.
4. FA – drusen close enough to disc surface will demonstrate autofluorescence. Early frames will demonstrate focal blockage of fluorescence. There may also be nodular late staining without leakage from disc surface capillaries.
5. CT scan is superior to MRI for detection of drusen (calcium produces bright signal at the optic nerve head).
25. What MRI technique allows better visualization of blood products, such as hemosiderin?
Specific T2 sequences (gradient echo) also allow better visualization of blood products, such as hemosiderin. These sequences are particularly helpful when evaluating patients with cerebral vascular malformations, tumors, trauma, or infarctions.
26. What is Isodense on CT?
Normal brain
27. What is hypodense on CT?
Edema, necrosis, and infarction.
28. What is hyperdense on CT?
Fresh blood, acute clot in a large vessel, bone, calcium, and fat.
29. What enhances with contrast on CT?
Blood vessels, inflammatory lesions, neoplasms, and the breakdown of the normal blood-brain barrier (e.g. from cerebral ischemia).
30. What are 7 good indications for CT?
1. Orbital trauma to rule out suspected fractures and foreign bodies.
2. Ocular trauma to rule out a foreign bodies and ruptured globe.
3. Infectious or noninfectious orbital inflammation.
4. Bone lesions (osteoma, fibrous dysplasia, suspected metastatic disease, etc.)
5. Preoperative imaging for orbital disease (when imaging of the facial sinuses is very important)
6. Lesions that may contain calcium (retinoblastoma, optic nerve drusen, orbital varix, meningioma, etc.)
7. Lacrimal gland lesions
31. What are 7 good indications for MRI?
1. Optic neuropathy
2. Suspected optic nerve tumor
3. Wooden foreign body
4. Orbital apex or cavernous sinus syndrome
5. Chiasmal syndrome
6. Brain lesion
7. Fungal sinusitis
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
4.6 Imaging of the Orbits and Visual Pathways
▶Table 4.1 presents the advantages and disadvantages of computed tomography (CT) and magnetic resonance (MR) for imaging the orbits and visual pathways.

4.6.1 Computed Tomography
Because bone, calcification, fat, and blood all have unique X-ray absorption patterns, CT is a very effective technique for orbital imaging (▶Table 4.2).
Specific absorption patterns can be highlighted on CT to emphasize bone, soft tissues, or blood.
CT images are classically obtained in the axial planes. It is possible to also request images in the coronal plane by repositioning the patient. Sagittal images may be obtained by computer reformatting.
Routine studies are done at 3 or 5mm slice intervals, but it is possible to obtain 1mm slice intervals (better resolution).
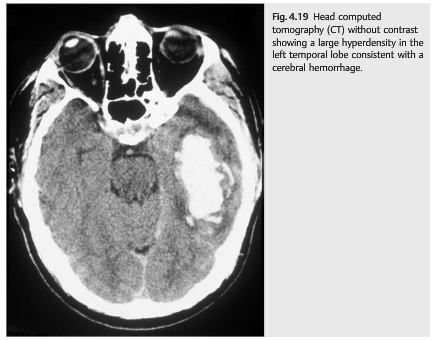
A head CT without contrast takes only a few minutes and is readily available. It is commonly performed in the emergency room and is extremely valuable in trauma patients (who may have a bone fracture or an orbital foreign body), in stroke patients (▶Fig. 4.19 and ▶Fig. 4.20), and when an acute intracranial or intraorbital hemorrhage is suspected (e.g., to detect a subarachnoid hemorrhage in a patient with an explosive headache).


However, a normal head CT without contrast is insufficient in almost all other situations. It is falsely reassuring and often misses serious disorders.
The following are good indications for orbital CT:
● Orbital trauma (suspected fractures or foreign body)
● Ocular trauma to rule out a foreign body (ruptured globe)
● Infectious or noninfectious orbital inflammation (▶Fig. 4.21 and ▶Fig. 4.22)
● Bone lesions (osteoma, fibrous dysplasia, suspected metastatic disease, etc.)
● Preoperative imaging for orbital disease (when imaging of the facial sinuses is very important)
● Lesions that may contain calcium (retinoblastoma, optic nerve drusen, orbital varix, meningioma, etc.)
● Lacrimal gland lesions


4.6.2 Magnetic Resonance Imaging
MRI offers many advantages over CT and is the most commonly obtained ancillary test in neuro-ophthalmology. It provides excellent contrast resolution between soft tissues, and multiplanar imaging can be done without repositioning the patient.
Various sequences are obtained that allow visualization of different tissues. The appearance of the tissues varies based on the sequence used.
T1-weighted images provide good anatomical details. Fat looks bright (hyperintense), vitreous looks black (hypointense), cerebrospinal fluid (CSF) looks black (hypointense), and subacute blood appears white (hyperintense). On T1-weighted images, brain gray matter is gray, and brain white matter is lighter. Most cerebral parenchymal lesions appear dark (hypointense), unless gadolinium contrast is given; in that case, and if there is a breakdown in the blood-brain barrier, they may appear white (hyperintense).
The T1-weighted midline sagittal view is the first sequence systematically obtained on MRI, and it is very helpful in neuro-ophthalmology (▶Fig. 4.23).
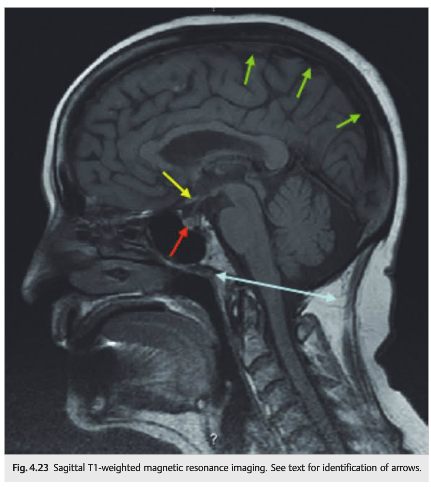
It provides information on the absence of cerebellar tonsillar herniation (Chiari malformation) (blue line in (▶Fig. 4.23), the pituitary gland (red arrow), the chiasm (yellow arrow), and the superior sagittal venous sinus (green arrows).
Because the orbits are filled with fat, a regular T1 sequence does not allow good evaluation of the orbits. In addition, administration of contrast results in enhancement of normal extraocular muscles and abnormal intraorbital structures; these appear brighter and therefore cannot be distinguished from the white orbital fat on a regular T1 sequence. A T1 sequence with fat suppression transforms the bright signal of the fat into a black signal and allows for very good orbital studies, before and after contrast administration (▶Fig. 4.24).

The orbits are best studied with a combination of axial and coronal views. Thin cuts are necessary.
Orbital MRI should include the following:
● Axial T1 sequence
● Axial T1 sequence with fat suppression
● Axial T1 sequence with fat suppression after injection of contrast
● Coronal T1 sequence with fat suppression
● Coronal T1 sequence with fat suppression after injection of contrast (▶Fig. 4.25)

T2-weighted images are ideal for screening for brain parenchymal abnormalities. OnT2-weighted images, fat looks darker (hypointense), vitreous looks bright (hyperintense), ventricles (CSF) look bright (hyperintense), and brain gray matter is lighter than brain white matter. Additionally, most cerebral parenchymal lesions appear bright (hyperintense), especially inflammatory or ischemic lesions.
Because the ventricles are filled with CSF, a regular T2 sequence shows the ventricles, and the subarachnoid space as very bright and does not allow for good evaluation of periventricular lesions, such as the white matter lesions from multiple sclerosis. A specific sequence called fluid-attenuated inversion recovery (FLAIR) allows transformation of the bright CSF signal into black signal, while maintaining the other characteristics of a T2-weighted image. FLAIR images are therefore “black CSF” T2-weighted images (▶Fig. 4.26).

Specific T2 sequences (gradient echo) also allow better visualization of blood products, such as hemosiderin. These sequences are particularly helpful when evaluating patients with cerebral vascular malformations, tumors, trauma, or infarctions.
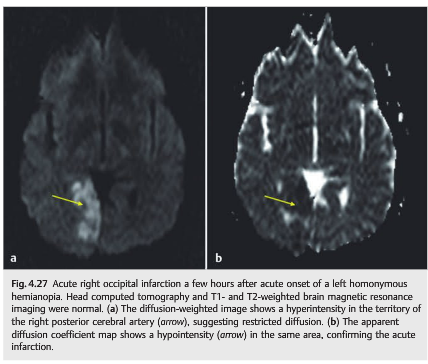
Diffusion-weighted images are ideal in detecting acute cerebral ischemia. They demonstrate restricted diffusion within hours of acute cerebral ischemia (while CT and other MRI sequences are often still normal) and should be obtained in all patients with acute neurologic deficits or when cerebral ischemia is suspected (▶Fig. 4.27).
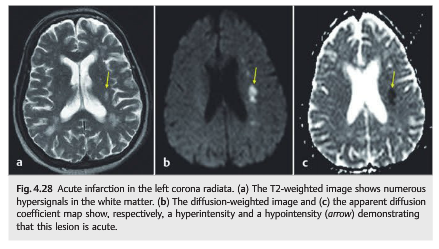
The appearance of lesions varies on diffusion-weighted images based on the time elapsed since the infarction. Old ischemic lesions do not show restricted diffusion, whereas acute ischemic lesions appear hyperintense on diffusion-weighted images and hypointense on the apparent diffusion coefficient (ADC) map (▶Fig. 4.28).
It is important to know which type of MRI to order. For example, with suspicion of cerebral infarction, a stroke protocol MRI of the brain should be ordered. This typically includes MRI without contrast (including sagittal T1-weighted sequence, axial T1-weighted sequence, axial FLAIR sequence, T2-weighted sequence, and often gradient echo to detect blood), MRI with diffusion-weighted images (shows very acute infarctions), and MRI with magnetic resonance angiography (MRA) of the head (circle of Willis) and neck (extracranial cervical arteries).
In the case of optic neuropathy, MRI of the brain and orbits with contrast should be ordered. This includes regular MRI of the brain with contrast (including sagittal T1-weighted sequence, axial T1-weighted sequence, axial FLAIR sequence, and T1- weighted sequence with contrast) and dedicated orbital views (including axial and coronal T1-weighted sequence with and without fat suppression, as well as axial and coronal T1-weighted sequence with fat suppression and with contrast).
In the case of chiasmal syndrome, the examiner should order an MRI scan of the brain and orbits with contrast, with special attention to the pituitary gland. T1, T2, and T1 axial, coronal, and sagittal views of the sella turcica and pituitary gland with contrast should also be ordered.
In the case of cranial nerve deficit, the examiner should order an MRI scan of the brain with contrast, with special attention to the specific cranial nerve. Imaging should also include very thin axial and coronal cuts in T1, T2, and T1 with contrast, covering the anatomical course of the cranial nerve in question.
The following are good indications for MRI:
● Optic neuropathy
● Suspected optic nerve tumor
● Wooden foreign body
● Orbital apex or cavernous sinus syndrome
● Chiasmal syndrome
● Brain lesion
● Fungal sinusitis
4.7 Vascular Imaging
Imaging of the intracranial and extracranial arteries and veins can be performed noninvasively with ultrasound, CT, and MRI. However, the gold standard for vascular imaging remains the catheter angiogram.
4.7.1 Vascular Ultrasound
Ultrasound allows reliable imaging of the extracranial carotid and vertebral arteries (▶Fig. 4.29 and ▶Fig. 4.30).
It combines Doppler imaging (which provides information on the flow within a blood vessel) and imaging of the vessels (often with color), thereby allowing quantification of the stenosis and evaluation of the hemodynamic significance of the stenosis. Transcranial Doppler (TCD) is used for evaluation of the intracranial cerebral circulation and of the ophthalmic artery. The transorbital, transtemporal, and transforaminal windows are used to detect flow within large intracranial arteries.

TCD is routinely used for detection of intracranial vessel stenosis, early identification of vasospasm in subarachnoid hemorrhage, and evaluation of intracranial hemodynamic impairment in patients with cervical artery stenosis and occlusion.
Doppler of the ophthalmic artery is helpful when there is ocular ischemia or to evaluate the collateral circulation in patients with severe carotid artery stenosis or carotid occlusion. It may show the following:
● Normal or attenuated flow in the ophthalmic artery
● No flow in the ophthalmic artery (indicating occlusion of the ophthalmic artery)
● Reversed flow in the ophthalmic artery (indicating that the ipsilateral cerebral anterior circulation is coming from branches of the external carotid artery in a patient with ipsilateral occlusion of the internal carotid artery). These patients have a high risk of hemodynamic cerebral infarction and chronic ocular ischemia.
4.7.2 Computed Tomographic Angiography and Venography
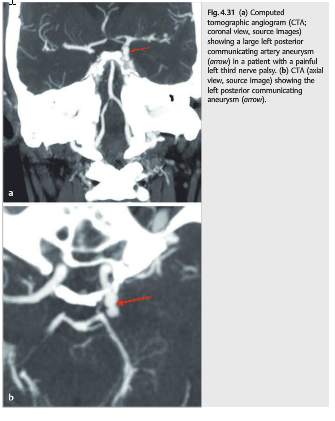
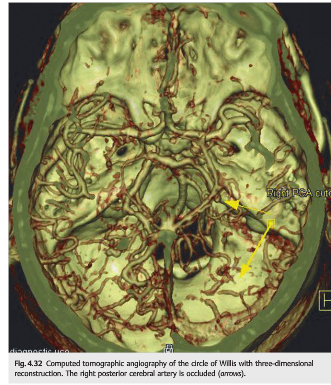
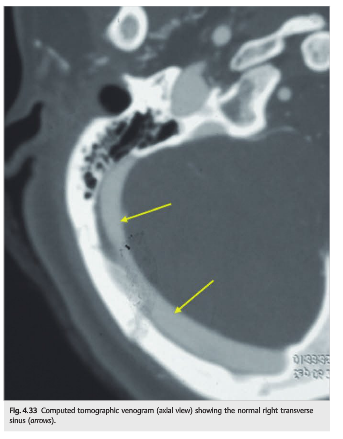
CT angiography (CTA) and CT venography (CTV) allow very good evaluation of the intracranial and extracranial arteries and veins. These tests require high volumes of contrast and may be problematic in patients with renal insufficiency or diabetes mellitus. Examination of the source images, as well as three-dimensional (3D) reconstructions, provides a very reliable screening for arterial stenosis, aneurysms, and venous stenosis or occlusion (▶Fig. 4.31, ▶Fig. 4.32, ▶Fig. 4.33).
4.7.3 Magnetic Resonance Angiography and Venography
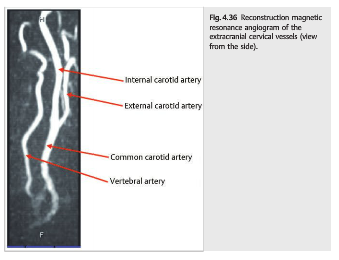
MR angiography (MRA) and MR venography (MRV) of the brain are often performed without contrast, although contrast can also be used with specific MRA and MRV techniques. The source images should be examined in addition to 3D reconstruction images (▶Fig. 4.34, ▶Fig. 4.35, ▶Fig. 4.36).


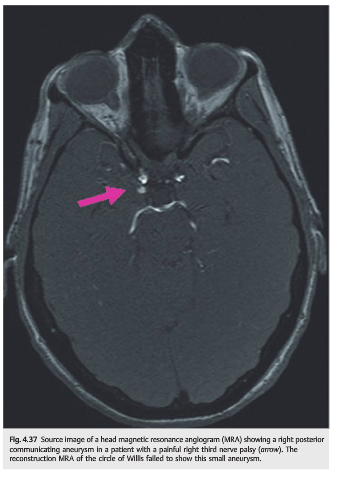
Interpretation of vascular imaging with MRA or CTA is difficult (▶Fig. 4.37). The radiologist often has to look at hundreds of images (the slice spacing is very small), and only a good clinical correlation allows accurate interpretation. Communication with the radiologist is essential.
4.7.4 Catheter Angiography
Catheter angiography is an invasive test that requires an experienced interventional radiologist. It is performed under local anesthesia and requires puncture of the femoral artery, along with selective catheterization of the cervical and intracranial arteries, with a catheter brought into the aorta. It also requires injection of a large volume of contrast.
Complications are rare when the test is performed by an experienced radiologist (<1% of procedures). However, the complications can be devastating and include the following:
● Groin hematoma
● Femoral artery pseudoaneurysm
● Aortic dissection
● Cervical artery dissection
● Disruption of atheromatous plaques present in the aorta with resultant distal emboli
● Cerebral infarction
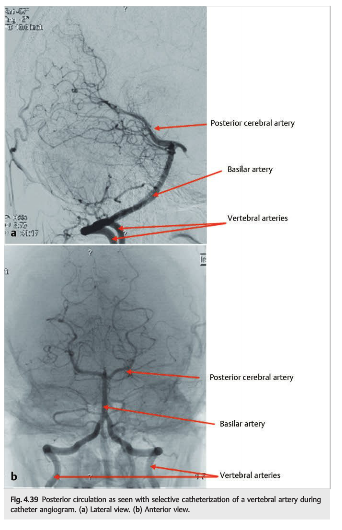
Despite advancement in noninvasive imaging, a catheter angiogram is still obtained in specific situations, such as carotid cavernous fistulas, aneurysms, and intracranial stenoses (▶Fig. 4.38 and ▶Fig. 4.39).

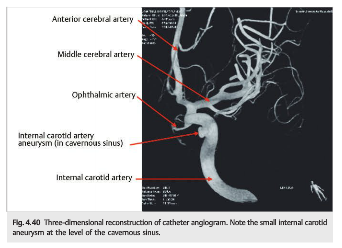
As for CTA, 3D reconstructions can be obtained with catheter angiography (▶Fig. 4.40). They allow better views of the circle of Willis as well as rotation of images. However, artifacts are possible, and these images should be correlated with conventional images.
Endovascular treatment of the aneurysm is often possible during the diagnostic catheter angiography performed emergently in a patient with a subarachnoid hemorrhage (▶Fig. 4.41a).
Whenever possible (depending on the location, the size and shape of the aneurysm, and the size and shape of its neck), the aneurysm is occluded with coils brought via the catheter used to perform the angiography. The coils promote thrombosis of the aneurysm sac (and therefore prevent rebleeding) and reduce the mass effect of the aneurysm.
The coils are made of platinum and are seen on plain X-ray (▶Fig. 4.41b). They produce artifact on CT or MRI scans, making subsequent noninvasive imaging of the brain and of the aneurysm difficult. It is thus usually necessary to obtain repeat catheter angiograms to image the intracranial vasculature in patients with a coiled aneurysm.

Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.