Questions:
45. What are the 4 most common neuro-ophthalmic manifestations of mitochondrial disorders?
46. Name 8 mitochondrial disorders with neuro-ophthalmic manifestations?
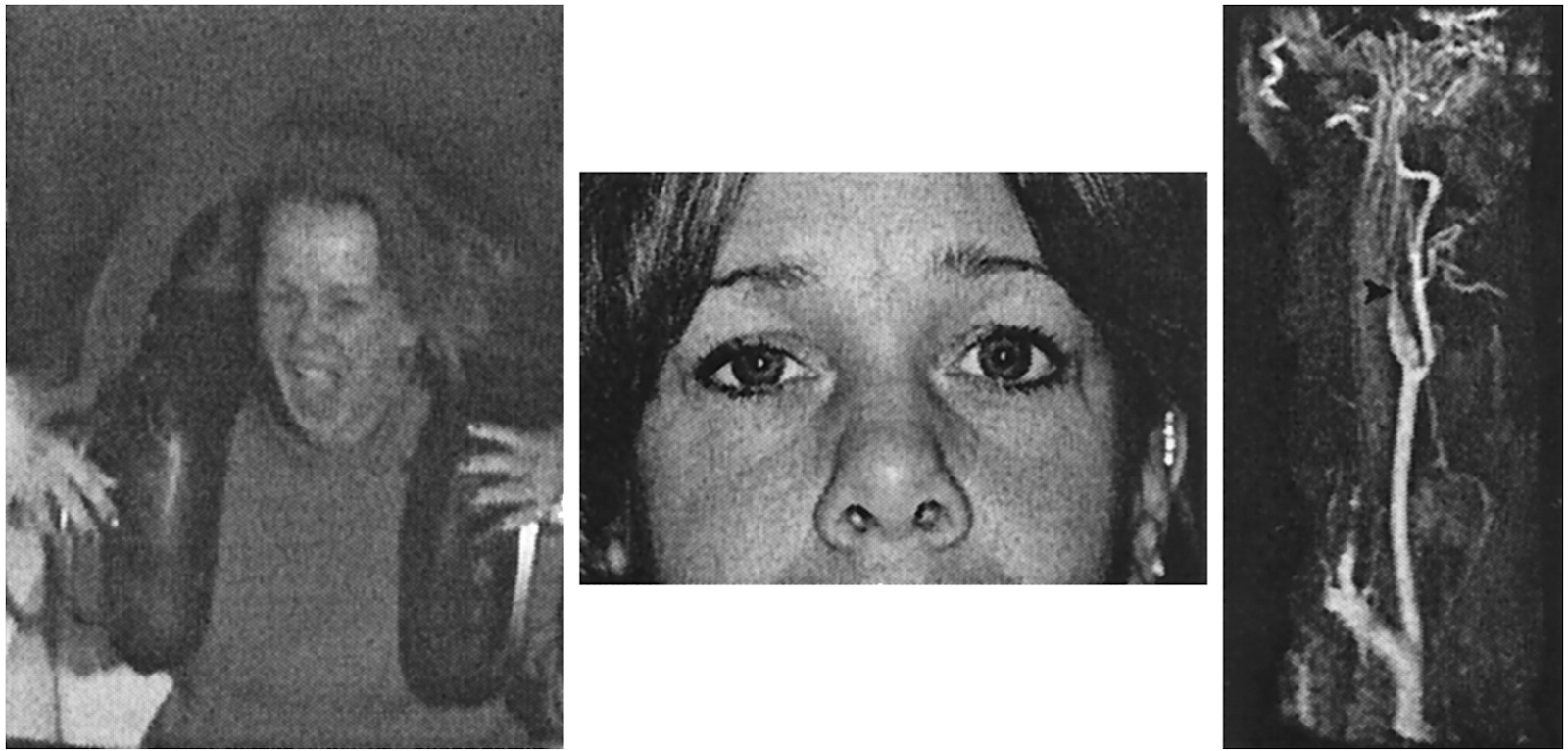
47. What are the ophthalmic and systemic manifestations of CPEO (chronic progressive external ophthalmoplegia)?
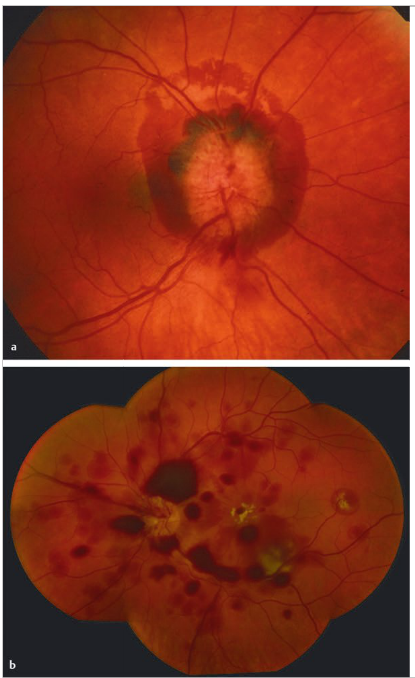
48. What are the ophthalmic and systemic manifestations of LHON (Leber hereditary optic neuropathy)?
49. What are the Chiari malformations?
50. What are the neuro-ophthalmic manifestations of the Chiari I malformation?
51. What are the ophthalmic manifestations of Parkinson?