Questions:
45. What are the 4 most common neuro-ophthalmic manifestations of mitochondrial disorders?
46. Name 8 mitochondrial disorders with neuro-ophthalmic manifestations?
47. What are the ophthalmic and systemic manifestations of CPEO (chronic progressive external ophthalmoplegia)?
48. What are the ophthalmic and systemic manifestations of LHON (Leber hereditary optic neuropathy)?
49. What are the Chiari malformations?
50. What are the neuro-ophthalmic manifestations of the Chiari I malformation?
51. What are the ophthalmic manifestations of Parkinson?
___________________________________
Questions with answers:
45. What are the 4 most common neuro-ophthalmic manifestations of mitochondrial disorders?
1. Bilateral optic neuropathy (Leber hereditary optic neuropathy or dominant optic atrophy)
2. Ophthalmoplegia with ptosis (chronic progressive external ophthalmoplegia)
3. Pigmentary retinopathy
4. Retrochiasmal visual loss (MELAS)
46. Name 8 mitochondrial disorders with neuro-ophthalmic manifestations?|
1. LHON (Leber hereditary optic neuropathy)
2. DOA (dominant optic atrophy)
3. CPEO (chronic progressive external ophthalmoplegia) & KSS (Kearns-Sayre syndrome)
4. MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes)
5. NARP (neurogenic muscle weakness, ataxia, and retinitis pigmentosa)/Leigh syndrome
6. MERRF (myoclonic epilepsy and ragged red fibers)
7. MIDD (maternally inherited diabetes mellitus and deafness)
8. MNGIE (mitochondrial neurogastrointestinal encephalomyopathy)
47. What are the ophthalmic and systemic manifestations of CPEO (chronic progressive external ophthalmoplegia)?
Ophthalmic – ophthalmoplegia, ptosis, and pigmentary retinopathy.
Systemic – myopathy ragged red fibers, peripheral neuropathy, deafness, vestibular dysfunction, basal ganglia lesions, cardiac conduction abnormalities, short stature, gastrointestinal dysmotility, delayed sexual maturation/hypogonadism, hypomagnesemia, hypoparathyroidism, and hypothyroidism.
48. What are the ophthalmic and systemic manifestations of LHON (Leber hereditary optic neuropathy)?
Ophthalmic: early disc microangiopathy, pseudo disc edema, vascular tortuosity, optic atrophy, Systemic: maternally inherited bilateral subacute optic neuropathy. Occasionally other features are present: tremor, a multiple sclerosis-like illness and cardiac conduction abnormalities, especially the pre-excitation syndromes. Additional findings that can occur in children include an extrapyramidal syndrome, seizures, ataxia, spasticity, mental retardation, and peripheral neuropathy. In the majority of patients with LHON, visual dysfunction is the only significant manifestation of the disease.
49. What are the Chiari malformations?
Chiari malformations represent a continuum of hindbrain maldevelopments characterized by downward herniation of the cerebellar tonsils. Chiari I malformation (Arnold-Chiari malformation) is defined as tonsillar herniation of at least 3 to 5 mm below the foramen magnum. It is sometimes associated with syringomyelia and other anomalies of the craniocervical junction. Chiari II and Chiari III malformations are present at birth and consist of downward herniation of the lower cerebellum and medulla into the spinal canal, in association with complex anomalies of the brain.
50. What are the neuro-ophthalmic manifestations of the Chiari I malformation?
Downbeat nystagmus & diplopia (unilateral or bilateral sixth nerve palsy/divergence insufficiency).
51. What are the ophthalmic manifestations of Parkinson?
● Decreased vision during reading and ocular discomfort
○ Ocular surface irritation
– Dry eyes
– Blepharitis
○ Decreased blink rate (hypokinesia)
○ Convergence insufficiency
● Impaired visual function
○ Decreased color discrimination
○ Decreased contrast sensitivity
○ Visuospatial deficits
● Visual hallucinations
● Abnormal eyelid movements
○ Reduced spontaneous blink
○ Blepharospasm
○ Apraxia of lid opening
● Abnormal eye movements
○ Decreased saccade performance
○ Decreased adaptive modification of saccade amplitudes
○ Ocular microtremor
○ Convergence insufficiency
● Complications of pallidotomy or stimulation
○ Contralateral homonymous hemianopia
○ Square-wave jerks
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
20.10 Mitochondrial Disorders
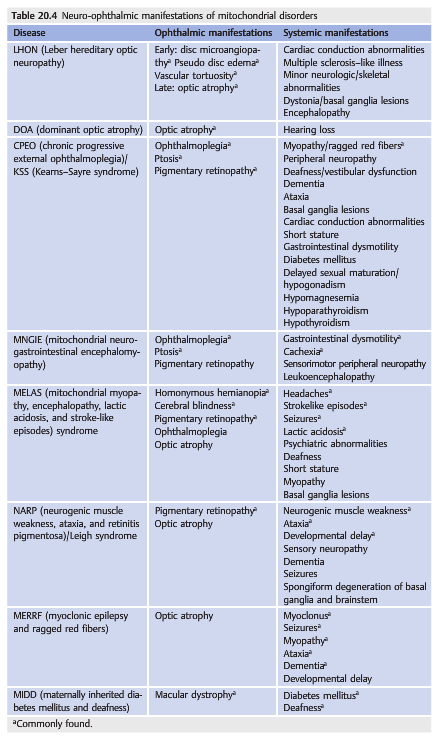
The mitochondrial diseases are a heterogeneous group of disorders in which clinical presentation, inheritance, histopathology, or biochemical or genetic analysis suggests primary mitochondrial dysfunction. In many of these disorders, the central nervous system and the eye figure prominently. ▶Table 20.4 lists the neuro-ophthalmic and systemic manifestations of several mitochondrial disorders.
The most common neuro-ophthalmic abnormalities seen in mitochondrial disorders include the following:
● Bilateral optic neuropathy (Leber hereditary optic neuropathy or dominant optic atrophy)
● Ophthalmoplegia with ptosis (chronic progressive external ophthalmoplegia)
● Pigmentary retinopathy
● Retrochiasmal visual loss (MELAS)
20.11 Chiari Malformations
Chiari malformations represent a continuum of hindbrain maldevelopments characterized by downward herniation of the cerebellar tonsils. Chiari I malformation (Arnold–Chiari malformation) is defined as tonsillar herniation of at least 3 to 5mm below the foramen magnum (▶Fig. 20.61).
It is sometimes associated with syringomyelia and other anomalies of the craniocervical junction.
There is overcrowding of the cerebellum within a small posterior cranial fossa leading to chronic tonsillar herniation. This overcrowding is believed to be responsible for the neurologic symptoms and signs that often develop during the second or third decade of life. Symptoms and signs may be related to changes in the CSF flow and to direct compression of the brainstem.
The clinical manifestations of Chiari I malformations are numerous, and it is often difficult to establish a direct relationship between nonspecific manifestations such as headache or dizziness and moderate tonsillar herniation.
● Often asymptomatic, discovered on a brain MRI obtained for another reason
● Headache (often with Valsalva or exercise)
● Dizziness, ataxia, vertigo
● Dysphagia, hoarseness
● Tinnitus
Neuro-ophthalmic manifestations of Chiari I malformations include the following:
● Downbeat nystagmus
● Diplopia
○ Unilateral or bilateral sixth nerve palsy
○ Divergence insufficiency
A specific MRI technique (Cine MRI) allows visualization of the CSF in the posterior fossa. The flow is abnormal in patients with symptomatic Chiari I malformation.
Treatment includes suboccipital decompression associated with C1 laminectomy and is performed only in patients with symptomatic Chiari I malformation.
Chiari II and Chiari III malformations are present at birth and consist of downward herniation of the lower cerebellum and medulla into the spinal canal, in association with complex anomalies of the brain.

20.12 Idiopathic Parkinson Disease
Although idiopathic Parkinson disease typically does not directly produce any clinically symptomatic ocular or neuro-ophthalmic complications, patients with idiopathic Parkinson disease have numerous ocular complaints, related either to the disease or to the medications used to treat the disease.
Neuro-ophthalmic manifestations of Parkinson disease include the following:
● Decreased vision during reading and ocular discomfort
○ Ocular surface irritation
– Dry eyes
– Blepharitis
○ Decreased blink rate (hypokinesia)
○ Convergence insufficiency
● Impaired visual function
○ Decreased color discrimination
○ Decreased contrast sensitivity
○ Visuospatial deficits
● Visual hallucinations
● Abnormal eyelid movements
○ Reduced spontaneous blink
○ Blepharospasm
○ Apraxia of lid opening
● Abnormal eye movements
○ Decreased saccade performance
○ Decreased adaptive modification of saccade amplitudes
○ Ocular microtremor
○ Convergence insufficiency
● Complications of pallidotomy or stimulation
○ Contralateral homonymous hemianopia
○ Square-wave jerks
Neuro-ophthalmic manifestations are also common with other Parkinson syndromes. For example, patients with Lewy body dementia often have terrifying visual hallucinations. Patients with supranuclear palsy have abnormal vertical eye movements early in the course of the disease.
Patients with Parkinson disease and similar syndromes may benefit from the following:
● Avoidance of medications that interact with tear secretion and accommodation
● Improved ambient light for reading to improve contrast
● Use of a music or cookbook stand to read if there is tremor or a downgaze deficit
● Treatment for ocular surface disease such as blepharitis
● Artificial tears
● Punctal occlusion for severe dry eye syndrome
● Avoidance of bifocals or progressive lenses
○ Increase the risk of a fall
○ Not correctly used if head bent over
○ Cannot be used with a walker ○ Increase asthenopia and diplopia
● Separate pairs of glasses for distance vision (walking and watching TV) and reading(reading and close-up work or eating)
● Base-in prism in reading glasses if symptomatic of convergence insufficiency
● When prescribing spectacles, the spherical equivalent may be preferable to significant astigmatic correction because glasses tend not to be stable on patients with tremor, dyskinesias, or susceptibility to falling.
● Using a finger to lead the eyes across the page in the setting of decreased saccadic velocity
● Treatment of blepharospasm and apraxia of eyelid opening with botulinum toxin and/or surgery if not improved after treatment of ocular surface irritation
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu .