Questions:
32. What type of iris nodules do the following have:
a. Neurofibromatosis Type 1
b, Neurofibromatosis Type 2
c. Uveitis?
33. A patient has infectious meningitis with severe papilledema. What risk does this pose and what should be done?
34. A patient presents with slowly progressive memory loss, cognitive impairment, oculomasticatory movements (myorhythmia), supranuclear vertical gaze palsy. What curable condition should be considered and what lab tests can be used to make the diagnosis?
35. What are 3 classic causes of raised ICP in a patient with known cancer?
36. What are neuro-ophthalmic manifestations of paraneoplastic syndromes?
37. What are the ocular manifestations of Neurofibromatosis Type 1?
38. What are the ocular or CNS manifestations of Neurofibromatosis Type 2?
39. What is the classic triad of findings in tuberous sclerosis?
40. What is the most prominent ocular manifestation of Tuberous sclerosis?
41. What autosomal dominant condition is associated with multiple, bilateral retinal angiomas and intracranial cerebellar hemangioblastomas?
42. What condition should be suspected with findings of telangiectasias of the conjunctival vessels and oculomotor apraxia?
43. A patient has an upper eyelid hemangioma, intraocular hypertension, and homonymous hemianopia, what condition is likely to be present?
44. What are the ocular manifestations of Sturge-Weber syndrome?
___________________________________
Questions with answers:
32. What type of iris nodules do the following have:
a. Neurofibromatosis Type 1: Lisch nodules (iris pigment epithelium hamartomas)
b. Neurofibromatosis Type 2: Lisch nodules and skin lesions are less common in NF2 than in NF1.
c. Uveitis: Iris nodules are an uncommon clinical sign in uveitis.
Busacca nodules lie on the iris surface and are pathognomonic for granulomatous uveitis.
Koeppe nodules (inflammatory cell precipitates) which lie at the pupillary margin and can be found in non-granulomatous as well as granulomatous uveitis.
The diseases most commonly associated with iris nodules and uveitis include sarcoidosis, Vogt-Koyanagi-Harada syndrome, multiple sclerosis, Fuchs heterochromic iridocyclitis, and metastatic infection.
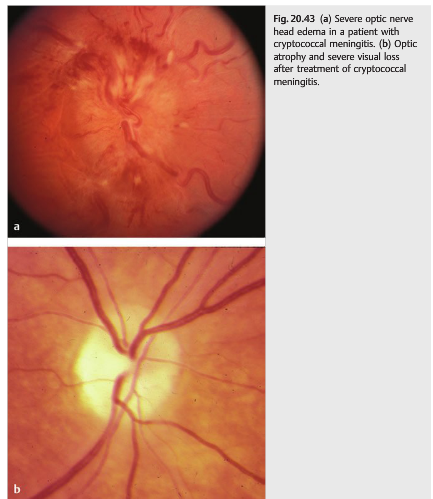
33. A patient has infectious meningitis with severe papilledema. What risk does this pose and what should be done?
Infectious meningitis often produces an increase in intracranial pressure and severe papilledema. Visual loss from unrecognized papilledema is a common cause of nonreversible visual loss in meningitis. Repeat lumbar punctures and other treatments for intracranial hypertension are crucial in this setting. Acute bacterial meningitis, tuberculous meningitis, and cryptococcal meningitis are particularly frequently associated with severe papilledema and visual loss.
34. A patient presents with slowly progressive memory loss, cognitive impairment, oculomasticatory movements (myorhythmia), supranuclear vertical gaze palsy. What curable condition should be considered and what lab tests can be used to make the diagnosis?
Whipple Disease: This rare disorder is often discussed in neuro-ophthalmology because it is frequently associated with eye movement abnormalities. It is caused by a gram-positive bacillus (Tropheryma whippelii), which mostly resides in the gut.
Diagnostic tests:
a. Positive polymerase chain reaction (PCR) for Tropheryma whippelii in the cerebrospinal fluid
b. Biopsy of jejunal mucosa with periodic acid-Schiff stain (PAS positive organisms)
c. Positive polymerase chain reaction (PCR) for Tropheryma whippelii in the jejunal biopsy.
Treatment consists of long-term antibiotics.
35. What are 3 classic causes of raised ICP in a patient with known cancer?
a. metastasis
b. carcinomatous meningitis
c. cerebral venous thrombosis (from a cancer-induced hypercoagulable state).
36. What are neuro-ophthalmic manifestations of paraneoplastic syndromes?
a. Abnormal eye movements – Opsoclonus (Ri antibodies), Ocular flutter (Ri antibodies), Cerebellar degeneration (Yo antibodies), Nystagmus, Slow saccades/limited vertical movements (Hu, Ma/Ta antibodies)
b. Neuromuscular junction disorder (Lambert Eaton or myasthenia) – Voltage-gated calcium channel antibodies
c. Visual loss: Cancer-associated retinopathy (CAR antibodies), Melanoma-associated retinopathy (MAR antibodies), Optic neuropathy with disc edema and intraocular inflammation (CRMP-5 antibodies)
37. What are the ocular manifestations of Neurofibromatosis Type 1?
Neurofibroma, Lisch nodules (iris pigment epithelium hamartomas), Optic nerve glioma, Sphenoid dysplasia (may cause pulsatile exophthalmos or enophthalmos, orbital encephalocele, orbital CSF)
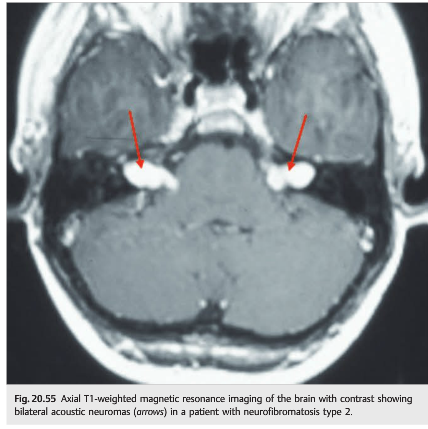
38. What are the ocular or CNS manifestations of Neurofibromatosis Type 2?
Unilateral or Bilateral eighth cranial nerve mass, Neurofibroma, Meningioma, Glioma, Schwannoma, Juvenile posterior subcapsular cataract, Lisch nodules, and skin lesions are less common in NF2 than in NF1. The most prominent manifestation of NF2 is bilateral acoustic neuromas.
39. What is the classic triad of findings in tuberous sclerosis?
Tuberous sclerosis is an autosomal dominant disorder, with high penetrance, and variable expressivity.
Patients present with a classic triad including:
a. Adenoma sebaceum
b. Mental retardation
c. Epilepsy
40. What is the most prominent ocular manifestation of Tuberous sclerosis?
The most prominent ocular manifestation is hamartoma of the retina and optic nerve. They are observed in up to 50% of patients but rarely cause visual loss. Seizures are the most common presenting symptom of tuberous sclerosis. Mental retardation occurs in more than 50% of these patients.
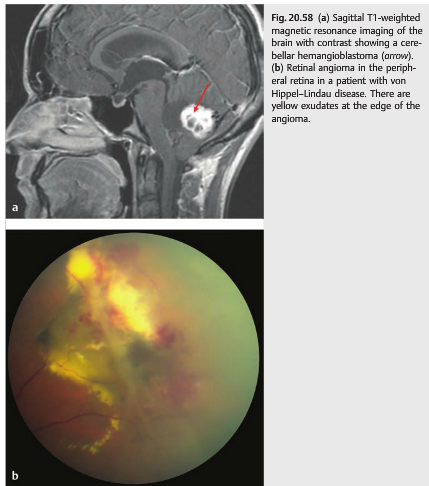
41. What autosomal dominant condition is associated with multiple, bilateral retinal angiomas and intracranial cerebellar hemangioblastomas?
Von Hippel Lindau disease is an autosomal dominant disorder associating multiple, bilateral retinal angiomas and intracranial hemangioblastomas (most often in the cerebellum). 25% of patients will have a renal cell carcinoma. 5% of patients will have a pheochromocytoma. The retinal angioma will typically have a feeder vessel, numerous exudates, and an exudative retinal detachment.
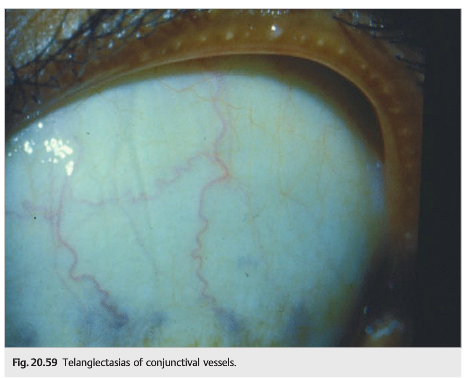
42. What condition should be suspected with findings of telangiectasias of the conjunctival vessels and oculomotor apraxia?
Ataxia telangiectasia is an autosomal recessive disorder associating cerebellar ataxia, telangiectasias, immunodeficiency, and susceptibility to neoplasms. Classic ophthalmologic manifestations are telangiectasias of the conjunctival vessels and oculomotor apraxia.
43. A patient has an upper eyelid hemangioma, intraocular hypertension, and homonymous hemianopia, what condition is likely to be present?
Sturge-Weber Syndrome (encephalotrigeminal angiomatosis) which is characterized by cutaneous hemifacial hemangioma associated hemangioma of the ipsilateral meninges and brain. It is a non-hereditary. In addition, there may be arteriovenous malformations, venous and dural sinus abnormalities.
44. What are the ocular manifestations of Sturge-Weber syndrome?
Intraocular hypertension (increased episcleral venous pressure, immature angle, and neovascularization of the angle). Glaucoma is particularly common when the hemangioma involves the upper eyelid. Angiomas are seen in the lid, conjunctiva, episclera and uvea. Associated findings include homonymous hemianopia contralateral to the meningeal hemangioma, seizures, headaches, and raised intracranial pressure.
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
20.5 Sarcoidosis
Sarcoidosis is a granulomatous inflammation that can affect every organ, particularly the lungs, the lymph nodes, the skin, and the eyes.
20.5.1 Patient Evaluation
Sarcoidosis may present with numerous systemic, neurologic, and neuro-ophthalmic symptoms and signs.
Most Common Presenting Symptoms of Sarcoidosis
● Respiratory symptoms in 50%
● Generalized symptoms (fatigue, fever, weight loss) in 20%
● Extrathoracic symptoms in 5 to 10%
● Asymptomatic (abnormal chest X-ray, abnormal liver function tests, hypercalcemia) in 20%
Clinical Manifestations of Sarcoidosis
● Pulmonary involvement in 90%
● Generalized symptoms (fatigue, fever, weight loss) in 20%
● Peripheral lymphadenopathy in 75%
● Cutaneous manifestations
● Liver involvement
● Neurologic manifestations in 5%
● Musculoskeletal manifestations in 5%
● Ocular involvement in 20%
● Cardiac dysfunction
● Renal manifestations
● Heerfordt syndrome (uveoparotid fever)
○ Uveitis
○ Parotid enlargement
○ Fever
○ Sometimes with seventh nerve palsy
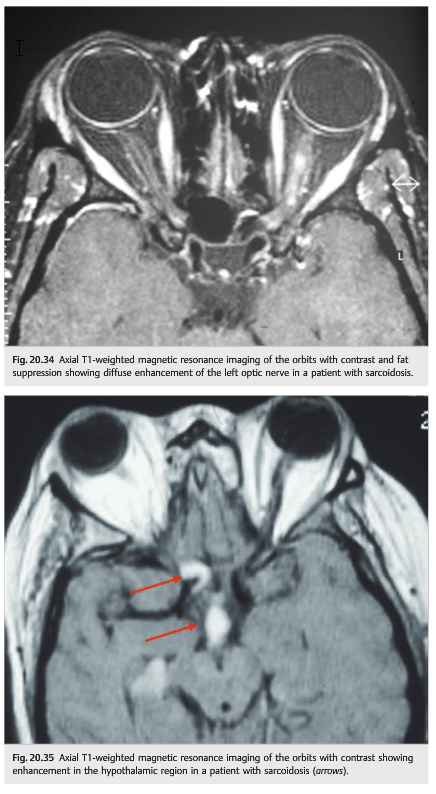
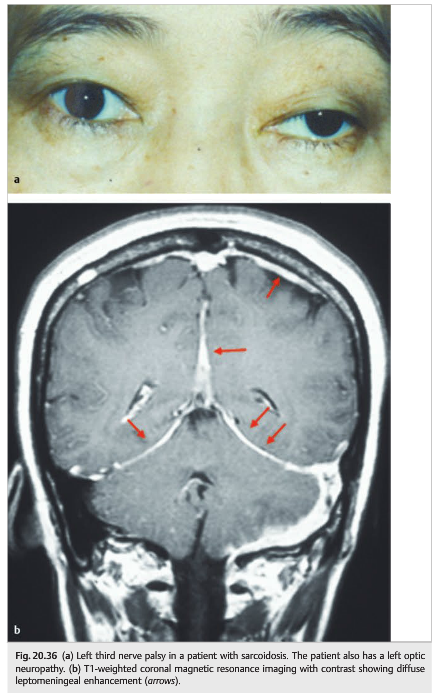
Neurologic manifestations of sarcoidosis (neurosarcoidosis), organized from the most common to the least common manifestation (▶Fig. 20.34, ▶Fig. 20.35, ▶Fig. 20.36), include the following:
● Cranial neuropathy
○ Seventh nerve palsy (facial weakness)
○ Eighth nerve palsy (deafness)
○ Ocular motor nerve (diplopia)
○ Optic neuropathy (optic neuritis)
● Aseptic lymphocytic meningitis
● Meningeal thickening (pachymeningitis)
● Hypothalamic dysfunction
● Intracranial mass (granuloma)
● Intraspinal mass (granuloma)
● Seizures
● Encephalopathy
● Peripheral neuropathy
Neuro-ophthalmic manifestations of systemic sarcoidosis are common, and systemic sarcoidosis may present with isolated ocular or neuro-ophthalmic manifestations ((▶Fig. 20.37, ▶Fig. 20.38 and ▶Fig. 20.39)



Ocular and neuro-ophthalmic manifestations of sarcoidosis, organized anatomically, include the following:
● Enlargement of the lacrimal gland
○ Pseudoptosis
○ Dry eye syndrome
● Anterior granulomatous uveitis
○ Visual loss
○ Intraocular hypertension
○ Posterior synechiae
○ Cataract
● Pars planitis (intermediate uveitis)
● Posterior uveitis
● Retinal vasculitis
● Retinal infiltrates (granuloma)
● Optic nerve granuloma
● Optic neuritis
● Chiasmal neuritis
● Papilledema (from raised intracranial pressure)
20.5.2 Diagnosis
Confirmation of the diagnosis of sarcoidosis may be difficult and is mostly aimed at identifying abnormal inflammatory tissue that can be biopsied.
● The gold standard is the histologic confirmation of sarcoid granulomas.
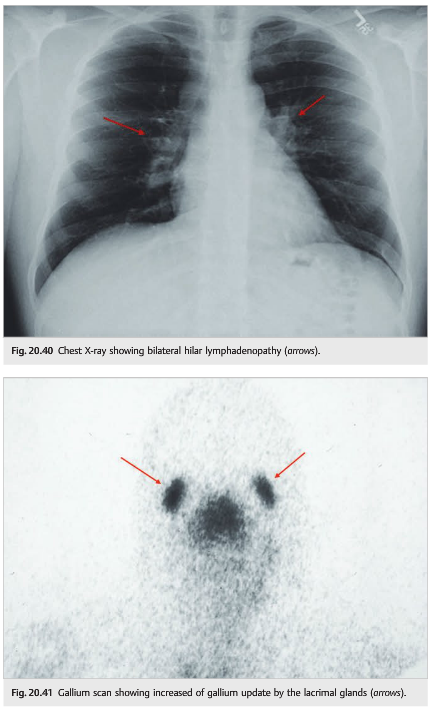
● Chest X-ray is the most useful screening and diagnostic test for sarcoidosis (▶Fig. 20.40).
○ Bilateral hilar adenopathy
○ Parenchymal infiltrates
● Chest CT
○ Early fibrosis
○ Hilar adenopathy
● Gallium scanning (▶Fig. 20.41)
○ Increased metabolic activity in the lungs; mediastinum; and lacrimal, parotid, and submandibular glands
● Whole body positron-emission tomography (PET) scan with fluorodeoxyglucose(FDG) is often used instead of a gallium scan
● Angiotensin-converting enzyme (ACE) in the blood
○ Often elevated in sarcoidosis (not specific)
● Hypercalcemia, hypercalciuria
● Cutaneous anergy to skin tests
● Bronchoalveolar lavage
○ Lymphocytosis in the bronchoalveolar lavage fluid
20.5.3 Treatment
● Sarcoidosis is classically very sensitive to steroids.
● In addition to local steroid treatment given for ocular complications of sarcoidosis (treatment of uveitis), systemic steroids are necessary. The dose, route, and duration of treatment depend on the severity of the manifestations.
● Neurosarcoidosis is usually treated more aggressively; other immunosuppressive treatments are usually necessary.
20.6 Infectious Diseases
Systemic infections can produce various neuro-ophthalmic manifestations. Infections can invade the intracranial space, the orbit, and the eye and can produce visual loss, visual field defects, and diplopia.
All infections (bacterial, viral, fungal, and parasitic) may invade the central nervous system and the eye, although some have a particular tropism for these organs. For example, cryptococcal infection (fungus) is a classic cause of acute meningitis in immunodeficient patients; secondary and tertiary syphilis (spirochete) are classic causes of meningitis, uveitis, and optic neuritis; zoster virus infection produces ocular signs and often ophthalmoplegia when involving the first branch of the trigeminal nerve; cat scratch disease (Bartonella henselae infection) is a classic cause of neuroretinitis.
The neurologic and ocular complications of systemic infections include the following:
● Intracranial infection
○ Cerebral abscess
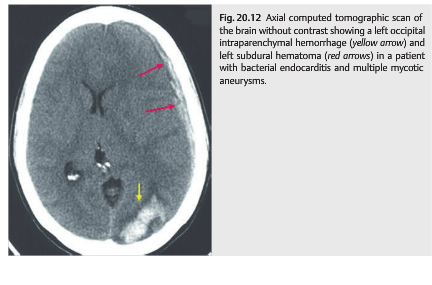
○ Cerebral empyema (▶Fig. 20.12)
○ Infectious meningitis
○ Optic neuritis
○ Encephalitis
○ Ventriculitis
○ Vasculitis
– Cerebral infarction
– Cerebral hemorrhages
○ Cavernous sinus abscess or thrombosis
● Orbital cellulitis
● Ocular infection
○ Endophthalmitis
○ Retinitis
○ Choroiditis
● Endocarditis
○ Cerebral infarction
○ Mycotic intracranial aneurysm
○ Retinal emboli (Roth spots)
● Cerebral venous thrombosis
○ Raised intracranial pressure (papilledema)
○ Venous infarction
Pearls
Infectious meningitis often produces an increase in intracranial pressure and severe papilledema. Visual loss from unrecognized papilledema is a common cause of non-reversible visual loss in meningitis. Repeat lumbar punctures and treatment of intracranial hypertension are crucial in this setting. Acute bacterial meningitis, tuberculous meningitis, and cryptococcal meningitis are particularly frequently associated with severe papilledema and visual loss.
20.6.1 Syphilis
Fig.20.42 Bilateral papilledema in a patient with secondary syphilis and chronic lymphocytic meningitis. This patient was found to be positive for HIV.


Neuro-ophthalmic complications of syphilis (▶Fig. 20.42) include the following:
● Uveitis (all types)
● Retinitis
● Choroiditis
● Optic neuritis
● Lymphocytic meningitis
○ Papilledema
○ Basilar meningitis with cranial nerve palsies
○ Vasculitis
– Cerebral infarction
● Intracranial mass (gumma)
20.6.2 Acquired Immunodeficiency Syndrome
Posterior segment manifestations of acquired immunodeficiency syndrome (AIDS) include the following (▶Fig. 20.43,▶Fig. 20.44,▶Fig. 20.45, ▶Fig. 20.46):



● Infectious
○ Herpes zoster ophthalmicus and optic neuritis
○ Herpes simplex optic neuritis
○ Progressive outer retinal necrosis (PORN)
○ Cytomegalovirus retinitis and optic neuritis
○ Toxoplasmosis chorioretinitis and optic neuritis
○ Syphilis retinitis and optic neuritis
○ Pneumocystis jiroveci (formerly P. carinii) choroiditis
○ Fungal choroiditis
○ Papilledema from meningitis (cryptococcal meningitis most common)
● Noninfectious
○ Retinal microvasculopathy
○ Retinal cotton wool spots
○ Ocular lymphoma
○ HIV optic neuritis
20.6.3 Cat Scratch Disease (Bartonella Henselae Infection)
Bartonella henselae infection produces various ocular manifestations, including anterior segment inflammation, retinitis, and optic neuritis (▶Fig. 20.47 and ▶Fig. 20.48). Retinal vascular occlusions are also common.
20.6.4 Whipple Disease
This rare disorder is often discussed in neuro-ophthalmology because it is frequently associated with eye movement abnormalities. It is caused by a gram-positive bacillus (Tropheryma whipplei), which mostly resides in the gut.
Clinical Presentation
● Weight loss, fever
● Diarrhea, abdominal pain
● Arthralgias
● Lymphadenopathy
● Neurologic manifestations (may be isolated):
○ Slowly progressive memory loss with cognitive impairment
○ Oculomasticatory movements (myorhythmia)
○ Supranuclear vertical (more than horizontal) gaze palsy
Diagnosis
● Positive polymerase chain reaction (PCR) for Tropheryma whipplei in the CSF
● Biopsy of jejunal mucosa with periodic acid-Schiff stain (PAS-positive organisms)
● Positive PCR for Tropheryma whipplei in the jejunal biopsy
Treatment
Treatment consists of long-term antibiotics.
Tumors
Intracranial tumors (all types) often produce neuro-ophthalmic symptoms and signs.
20.6.5 Mechanisms
The mechanisms by which brain tumors produce neuro-ophthalmic symptoms and signs include the following.
● Raised intracranial pressure (from the mass or from obstructive hydrocephalus)
○ Papilledema
○ Diplopia (from sixth nerve palsy)
● Mass effect or infiltration
○ Choroidal metastasis
○ Intracranial optic nerve (optic neuropathy)
○ Chiasm (bitemporal hemianopia)
○ Retrochiasmal visual pathways (homonymous hemianopia)
○ Ocular motor cranial nerve (diplopia)
● Carcinomatous meningitis
○ Raised intracranial pressure
○ Multiple cranial nerve palsies
● Paraneoplastic syndrome from a cancer
○ Retinopathy
○ Optic neuropathy
○ Nystagmus, opsoclonus, brainstem syndromes
● Toxicity of treatment
○ Postsurgical complication
○ Radiation
– Radiation necrosis of the brain
– Radiation optic neuropathy (see Chapter 8)
– Radiation retinopathy
○ Chemotherapy
– Optic nerve toxicity
Cancer patients who develop neuro-ophthalmic symptoms or signs (such as optic neuropathy, papilledema, visual field defect, diplopia, or nystagmus) need immediate neuroimaging (MRI of the brain, often with the orbits, and with contrast). If the imaging is normal, then a lumbar puncture with CSF opening pressure, cytology, and flow cytometry need to be performed.
20.6.6 Carcinomatous Meningitis
Carcinomatous meningitis must be ruled out in all patients with raised intracranial pressure and a known history of cancer. Imaging is often normal or may show leptomeningeal enhancement. A lumbar puncture with CSF opening pressure and CSF analysis, including cytology and flow cytometry, is mandatory. If normal, the lumbar puncture should be repeated for repeat cytologic examination. Sometimes, it is necessary to perform at least three lumbar punctures to make a diagnosis of carcinomatous meningitis.
The most common sites or types of cancer in patients with carcinomatous meningitis are as follows:
● Breast
● Lung
● Lymphoma
● Melanoma
● Adenocarcinoma of unknown origin


Pearls
The three classic causes of raised intracranial pressure in patients with known cancer are (1) metastasis, (2) carcinomatous meningitis, (3) cerebral venous thrombosis (from cancer-induced hypercoagulable state).
20.6.7 Paraneoplastic Syndromes
Paraneoplastic syndromes represent rare nonmetastatic complications of cancer, which can affect multiple levels of the nervous system. Autoantibodies are usually found in the CSF or serum. Paraneoplastic syndromes may complicate a known cancer or may be the first sign of a very localized cancer.
Neuro-ophthalmic symptoms and signs are relatively common and include the following:
● Abnormal eye movements
○ Opsoclonus (Ri antibodies)
○ Ocular flutter (Ri antibodies)
○ Cerebellar degeneration (Yo antibodies)
○ Nystagmus
○ Slow saccades, limited vertical movements (Hu, Ma/Ta antibodies)
● Neuromuscular junction disorder (Lambert–Eaton syndrome or myasthenic syndrome)
○ Voltage-gated calcium channel antibodies
● Visual loss
○ Retinal degeneration
– Cancer-associated retinopathy (CAR) antibodies
– Melanoma-associated retinopathy (MAR) antibodies
○ Optic neuropathy with disc edema and intraocular inflammation
– CRMP-5 antibodies
20.7 Traumatic Brain Injury
Neuro-ophthalmic manifestations of traumatic brain injury include the following:
● Visual loss
○ Monocular
– Trauma to the eye
– Orbital trauma
– Optic nerve injury (direct/indirect)
○ Binocular
– Trauma to both eyes or both optic nerves
– Traumatic chiasmopathy (bitemporal hemianopia)
– Trauma to the retrochiasmal visual pathways (homonymous hemianopia)
○ Higher cortical function impairment from brain injury
● Diplopia
○ Orbital trauma (entrapment, fibrosis of extraocular muscles)
○ Cranial nerve palsies (fourth, sixth, and third)
○ Intracranial lesions
Causes of posttraumatic acute visual loss include the following:
● Refractive error
○ Glasses or contact lenses are lost or damaged at the time of trauma (may be overlooked in patients with difficulty communicating)
● Ocular injury
○ Ruptured globe (anterior with corneal laceration or posterior with scleral laceration)
○ Intraocular foreign body
○ Exposure keratopathy (secondary to proptosis, lid laceration, or seventh nerve dysfunction)
○ Corneal edema (from airbag injury)
○ Corneal abrasion
○ Hyphema (blood in anterior chamber)
○ Traumatic iritis (often delayed by about 24 hours)
○ Traumatic mydriasis (and decreased accommodation)
○ Lens subluxation or luxation
○ Vitreous hemorrhage
○ Commotio retinae
○ Retinal detachment
○ Retinal ischemia from carotid dissection
○ Retinal fat emboli
○ Choroidal rupture
● Optic nerve
○ Direct traumatic optic neuropathy
○ Indirect traumatic optic neuropathy
○ Intrasheath hematoma
○ Avulsion of the optic nerve head
○ Penetrating injuries of the orbit with direct optic nerve injury
○ Intraorbital foreign body
○ Optic nerve ischemia from carotid dissection
● Orbit
○ Orbital fracture (direct optic nerve damage)
○ Orbital hemorrhage (optic nerve ischemia)○ Orbital emphysema (optic nerve ischemia)
○ Carotid cavernous fistula (increased intraocular pressure)
○ Subperiosteal hemorrhage (direct optic nerve damage or optic nerve ischemia)
● Intracranial optic pathways
○ Chiasmal or retrochiasmal direct injury
○ Chiasmal or retrochiasmal indirect injury
○ Hemorrhage or hematoma compressing the chiasm
○ Cerebral diffuse axonal injury with homonymous hemianopia
○ Intraparenchymal hemorrhage with homonymous hemianopia
○ Cerebral infarction (posterior cerebral artery) secondary to increased intracranial pressure/herniation with homonymous hemianopia or cerebral blindness
○ Cerebral infarction secondary to cervical artery dissection with homonymous hemianopia
20.8 Visual Loss during Ocular or Cranial Surgery
Damage to the intracranial visual pathways or to the optic nerves may occur during surgery. Visual loss is particularly common during ocular and intracranial surgery, but it may occur as a complication of any surgical procedure. The first step when evaluating a patient with postoperative visual loss is to localize the lesion by an ophthalmic examination.
Visual loss during ocular surgery can result from the following:
● Optic neuropathy
○ Direct damage to the retrobulbar optic nerve from retrobulbar anesthesia, orbital surgery, orbital hemorrhage after blepharoplasty
○ Fluctuation in intraocular pressure during ocular surgery
○ Postoperative intraocular hypertension
● Diplopia
○ Direct damage to the extraocular muscles from the following:
– Retrobulbar anesthesia
– Orbital surgery
– Orbital hemorrhage after blepharoplasty
– Scleral buckle placed for treatment of a retinal detachment
● Ptosis
○ Damage of the levator muscle from the ocular speculum
Visual loss during cranial surgery can result from compression, edema, ischemia, hemorrhage, or direct injury to the intracranial optic nerve, the chiasm, or the intracranial retrochiasmal visual pathways.
Visual loss during nonocular, noncranial surgery can result from the following:
● Anterior segment lesion
○ Corneal abrasion
○ Trauma (pressure on the eye during surgery)
○ Reversible retinal toxicity after prostate surgery (irrigating solution)
● Ocular ischemia
○ Central retinal artery occlusion
○ Ischemic optic neuropathy (anterior and posterior)
● Chiasmal lesion
○ Pituitary apoplexy
● Intracranial ischemia (homonymous hemianopia or cerebral blindness)
Ischemic optic neuropathies are particularly common after coronary artery bypass graft and after spinal surgery. Their mechanism remains debated.
Retinal and optic nerve ischemia may also occur during any procedure complicated by major bleeding with severe hypotension and after procedures involving the cervical vessels or dissection of the neck.
20.9 Phacomatoses
The phacomatoses are a group of disorders characterized by multiple hamartomas of the central and peripheral nervous systems, eye, skin, and viscera. The central nervous system lesions in phacomatoses have a very different natural history and prognosis than those found in other patients (e.g., the gliomas observed in the phacomatosis neurofibromatosis type 1 are often benign, whereas a glioma in a patient without neurofibromatosis may be a more aggressive tumor).
20.9.1 Neurofibromatosis Type 1
Neurofibromatosis type 1 (NF1; also known as von Recklinghausen disease) is the most common phacomatosis (1/5,000) and is autosomal dominant (NF1 gene localized on chromosome 17) with high penetrance and variable expressivity.
The diagnostic criteria for NF1 include two or more of the following:
● Café au lait macules (≥ 6) (▶Fig. 20.49)
● Neurofibromas (≥2) (▶Fig. 20.50 and ▶Fig. 20.51)
● Freckling (axillary, inguinal)
● Lisch nodules (iris pigment epithelium hamartomas) (▶Fig. 20.52)
● Optic nerve glioma (▶Fig. 20.53)
● Sphenoid dysplasia (▶Fig. 20.54)
● First-degree relative with NF1






The most prominent manifestation of NF1 is the involvement of cranial and peripheral nerves by two types of tumors:
● Schwannomas (neuromas, neurinomas, neurilemmomas)
○ Affect cranial nerves (fifth, third, fourth, and sixth nerves are most commonly affected)
● Neurofibromas
○ Plexiform neurofibromas
○ Localized neurofibromas
Central nervous system tumors (see ▶Fig. 20.53) are common in NF1.
● Optic nerve or chiasmal gliomas (in 15–20% of NF1 patients)
○ Often asymptomatic
○ May produce progressive loss of vision
○ May improve spontaneously
○ Treatment (chemotherapy, radiation) is performed only in cases with documented worsening of visual function.
● Low-grade astrocytic tumors
● Pulsatile exophthalmos or enophthalmos
● Herniation of dura, CSF, and brain into the orbit (encephalocele)
● May rarely result in compression of the extraocular muscles with diplopia and compression of the optic nerve with visual loss

Patients with NF1 may also have sphenoid dysplasia or absence of the sphenoid wing (see ▶Fig. 20.54).
20.9.2 Neurofibromatosis Type 2
Neurofibromatosis type 2 (NF2) is much less common than NF1 (1/50,000) and is an autosomal dominant disorder (NF2 gene localized on chromosome 22) with high penetrance.
The diagnostic criteria for NF2 include the following:
● Bilateral eighth cranial nerve mass identified on imaging or first degree relative with NF2 and
● Unilateral eighth nerve mass or two or more of the following:
○ Neurofibroma
○ Meningioma
○ Glioma
○ Schwannoma
○ Juvenile posterior subcapsular cataract
● Lisch nodules and skin lesions are less common in NF2 than in NF1.
● The most prominent manifestation of NF2 is bilateral acoustic neuromas (▶Fig. 20.55).

20.9.3 Tuberous Sclerosis (Bourneville disease)
Tuberous sclerosis is an autosomal dominant disorder, with high penetrance, and variable expressivity.
Patients present with a classic triad including the following:
● Adenoma sebaceum
● Mental retardation
● Epilepsy
Diagnosis
Definite diagnosis requires one primary feature and two secondary features or one secondary feature and two tertiary features.
● Primary features
○ Facial angiofibromas (▶Fig. 20.56)
○ Multiple ungual fibromas
○ Cerebral mass: cortical tubers, giant cell astrocytoma, calcified subependymal nodules protruding in the ventricle
○ Multiple retinal astrocytomas (▶Fig. 20.57)
● Secondary features
○ Affected first-degree relative
○ Cardiac rhabdomyosarcoma
○ Retinal hamartoma or retinal achromatic patch
○ Shagreen patch
○ Forehead plaque
○ Pulmonary lymphangiomyomatosis
○ Renal angiomyolipoma, renal cysts
● Tertiary features
○ Hypomelanotic macules
○ “Confetti” skin lesions
○ Renal, bone cysts
○ Nonrenal angiomyolipoma
○ Hamartomatous rectal polyps
○ Pulmonary lymphangiomyomatosis
○ Gingival lipomas
○ Infantile spasms
○ Cerebral white matter migration tracts or heterotopias


Seizures are the most common presenting symptom of tuberous sclerosis.
Mental retardation occurs in>50% of patients.
The most prominent ocular manifestation is hamartomas of the retina and optic nerve. They are observed in up to 50% of patients but rarely cause visual loss.
20.9.4 Von Hippel–Lindau Disease
Von Hippel–Lindau disease is an autosomal dominant disorder associating multiple, bilateral retinal angiomas and intracranial hemangioblastomas (most often in the cerebellum) (▶Fig. 20.58).
Twenty-five percent of patients will have a renal cell carcinoma. Five percent of patients will have a pheochromocytoma.
● Retinal angioma
○ Feeder vessel
○ Numerous exudates
○ Exudative retinal detachment
20.9.5 Ataxia Telangiectasia (Louis-Bar Syndrome)
Ataxia telangiectasia is an autosomal recessive disorder associating cerebellar ataxia, telangiectasias, immunodeficiency, and susceptibility to neoplasms. Classic ophthalmologic manifestations include the following:
● Telangiectasias of the conjunctival vessels (▶Fig. 20.59)
● Oculomotor apraxia
20.9.6 Sturge-Weber Syndrome (Encephalotrigeminal Angiomatosis)

● Characterized by cutaneous hemifacial hemangioma associated with hemangioma of the ipsilateral meninges and brain (▶Fig. 20.60)
● Nonhereditary disorder
● Facial hemangioma present at birth (follows V1 and V2 innervation)
● Ocular manifestations ipsilateral to the hemangioma
○ Intraocular hypertension (increased episcleral venous pressure, immature angle, and neovascularization of the angle); glaucoma is particularly common when the hemangioma involves the upper eyelid.
○ Choroidal hemangioma
● Homonymous hemianopia contralateral to the meningeal hemangioma
● Seizures, headaches are common
● Raised intracranial pressure possible
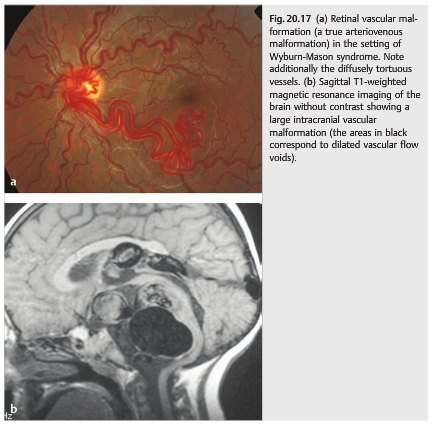
20.9.7 Wyburn-Mason Syndrome
● Association of retinal arteriovenous malformations with an intracranial arteriovenous malformation, typically in the ipsilateral brainstem (see Fig. 20.17).
● Nonhereditary
20.9.8 Klippel-Trénaunay-Weber Syndrome
● Large cutaneous hemangiomas with hypertrophy of the related bones and soft tissues
● Retinal angiomas
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu .