Questions:
Nystagmus Basics
1. What 14 features should be assessed in the evaluation of a patient with nystagmus?
2. What are the characteristics of physiologic nystagmus?
3. What are the characteristics, lesion locations, associated conditions, concerns, and treatment for peripheral vestibular nystagmus?
4. What are the characteristics, lesion locations, associated conditions, and concerns for central nystagmus?

_____________________________________________
Questions with answers:
1. What 14 features should be assessed in the evaluation of a patient with nystagmus?
1. Physiologic or pathologic
2. Infantile or acquired
3. Peripheral or central
4. Pendular or jerk
5. Symmetry: conjugate or disconjugate (dissociated)
6. Directions: horizontal, vertical, torsional
7. Amplitude
8. Frequency
9. Effect of fixation
10. Oscillopsia
11. Vertigo
12. Head movements
13. Hearing loss, tinnitus
14. Presence of additional neurologic signs
2. What are the characteristics of physiologic nystagmus (rapid gaze-evoked nystagmus)?
1. Present only in extremes of horizontal gaze.
2. Horizontal and dampens within seconds.
3. Symmetric in left and right gaze.
4. Resolves when the eyes are in a slightly less eccentric position.
Other findings indicate pathologic nystagmus.
3. What are the characteristics, lesion locations, associated conditions, concerns, and treatment for peripheral vestibular nystagmus?
Characteristics
– Horizontal, mixed horizontal/torsional, sometimes vertical component.
– Fast phase away from the lesion.
– Fixation inhibits.
– Increases with Frenzel goggles or darkness.No associated eye movement deficits.
– Often induced by head movements.
– Dix-Hallpike patency present, duration < 1 minute, fatigues, reversal with upright position.
Locations
– Unilateral: disease of vestibular organ or nerve.
– Bilateral disease of vestibular organ and nerve (usually drug toxicity) doesn’t produce nystagmus but produces loss of the vestibulo-ocular reflex.
Associated conditions Hearing loss.
Concerns Usually benign disease: labyrinthitis, Ménière disease.
Treatment BPPV does not respond well to medications but may have a long-term favorable response to numerous maneuvers aimed at dislodging the debris from the posterior semicircular canal.
4. What are the characteristics, lesion locations, associated conditions, and concerns for central nystagmus?
Characteristics
– Does not fatigue or reverse with upright position.
– Torsional pure. Vertical pure. Horizontal pure.
– Direction of nystagmus may change with gaze.
– No inhibition with fixation.
– Frenzel goggles or darkness (inhibition of fixation) no change in nystagmus.
– Associated eye movement defects:
– May have pursuit or saccadic defects.
– May have cranial nerve or long tract signs.
– No tinnitus or hearing loss.
– Associated eye movement defects: mild (except for Wallenberg syndrome).
– Dix-Hallpike: no latency, duration > 1 minute, does not fatigue, does not reverse with upright position.
Associated conditions Any CNS Disorder
Locations/Concerns Disease of the brainstem and its connections with the vestibulocerebellum
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ1
16 Nystagmus and Other Ocular Oscillations
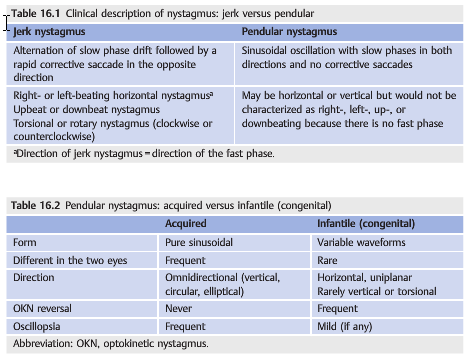
Nystagmus is a rhythmic, repetitive oscillation of the eyes, initiated by a slow eye movement that drives the eye o target, followed by a fast movement that is corrective(jerk nystagmus) or another slow eye movement in the opposite direction (pendular nystagmus). Saccadic intrusions (opsoclonus and flutter) are abnormal rapid eye movements (saccades) that have no slow phase. All such eye movements disrupt fixation and may interfere with vision.
16.1 Nystagmus
Nystagmus may occur physiologically in response to an environmental stimulus or change in body position. It is also seen with diseases of the central nervous system or peripheral vestibular system and in some cases of visual loss. Physiologic nystagmus or rapid gaze-evoked nystagmus is present only in extremes of horizontal gaze and dampens within seconds. It resolves when the eyes are in a slightly less eccentric position. Pathologic nystagmus is characterized as jerk or pendular, and infantile (congenital)or acquired. In patients presenting with nystagmus and vertigo, it is essential to differentiate peripheral vestibular nystagmus from central nystagmus (▶Table 16.1, ▶Table 16.2, ▶Table 16.3, ▶Table 16.4, ▶Table 16.5).


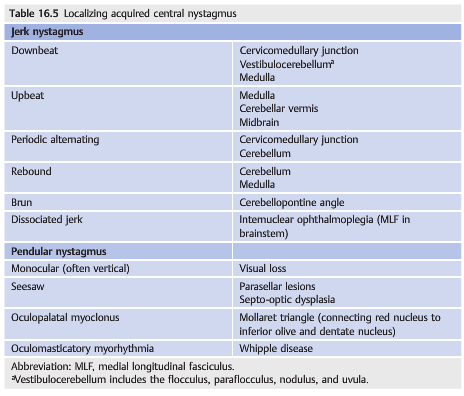
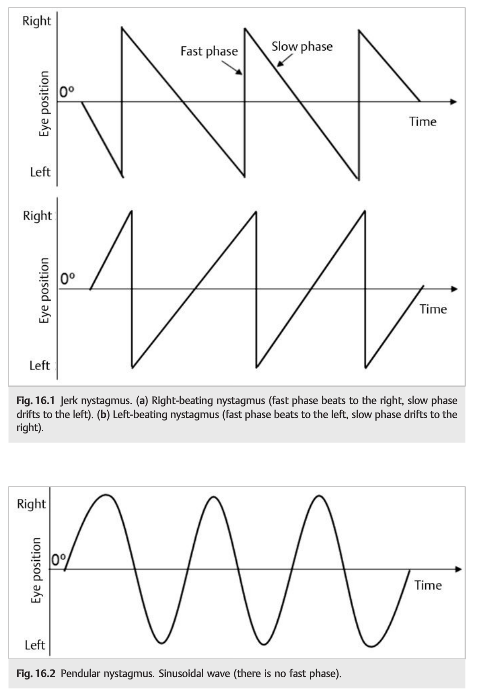
Most patients with nystagmus complain of oscillopsia (oscillating vision with illusion that objects are moving), and in most cases, nystagmus can be recognized clinically without eye movement recording. However, eye movement recording allows far more accurate characterization of the nystagmus by analyzing the slow phase (velocity, amplitude, and frequency) (▶Fig. 16.1 and ▶Fig.6.2) show the waveforms of horizontal jerk and pendular nystagmus.
16.1.1 Patient Evaluation
The goals of the evaluation are to decide whether there is a central or peripheral pattern of nystagmus and to determine if localization is possible based on the findings(▶Table 16.3 and ▶Table 16.4). Symptoms include oscillopsia (absent in congenital nystagmus), decreased acuity, nausea or vomiting, and vertigo.
There may be coexisting neurologic deficits.
The examination (in primary position as well as all positions of gaze) differentiates jerk from pendular nystagmus. If the finding is jerk nystagmus, look for the direction of the fast phase—watch for a few minutes, as nystagmus may occasionally alternate directions. Look for coexisting head oscillations or head turns, the effect of convergence on nystagmus, the presence of a null point (eye position where nystagmus is least prominent), and subtle nystagmus or vestibular nystagmus that is suppressed by fixation. The last can be assessed by performing ophthalmoscopy in one eye while the patient fixates at distance, then covering the fixating eye. Nystagmus may then be viewed through the ophthalmoscope (the fast phase direction is the opposite of what it appears through the direct ophthalmoscope). Frenzel goggles may be used to assess nystagmus in the absence of fixation. Electronystagmography (ENG) is another method of identifying nystagmus not present with eyes open. Finally, the Dix–Hallpike or Bárány maneuver can be done to look for positional nystagmus in patients who complain of positional vertigo (see ▶Table 16.4; ▶Fig. 16.3).

“The Dix-Hallpike test can help distinguish central vertigo from peripheral vertigo. During the test, the clinician rotates the patient’s head 45 degrees to one side and then helps the patient to quickly lie back down. If rotational nystagmus is observed, the test is considered positive for benign positional vertigo. If the test is negative, CNS dysfunction may be indicated.”2
Reference:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
2. Medscape – Central Vertigo Clinical Presentation
https://emedicine.medscape.com/article/794789-clinical?pa=bDt2d0GDhhy%2Bgp6U4l17r0x8KbiFmG7siR1UQzvHgOizSipHPzJXI0PSbqe3fzjm#showall
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.