Questions:
71. What should the findings of AION in the absence of a small crowded optic nerve head with a small cup-to-disk ratio suggest?
72. Which is more likely to have pain, nonarteritic AION or Arteritic AION
73. If the reduction of visual acuity is small in nonarteritic AION, how is color vision likely to be affected?
74. What kind of process is believed to be present in diabetic papillopathy?
75. How is diabetic papillopathy distinguished from typical nonarteritic AION?
76. Is nonarteritic AION associated with ipsilateral internal carotid artery stenosis?
77. What are 9 risk factors for nonarteritic AION?
78. Should the internal carotid arteries be evaluated in nonarteritic AION?
79. Is there an increased risk of cerebrovascular disease in the population of patients with AION?
80. Does the presence of optic nerve head drusen or papilledema increase the risk of nonarteritic AION?
81. What medication may induce an optic neuropathy that mimics nonarteritic AION?
82. Is there a proven treatment for nonarteritic AION?
83. What conditions are associated with nonarteritic PION?
84. How is nonarteritic PION diagnosed?
Neuro-ophthalmology Illustrated Chapter 8 – Optic Neuropathies 6
Neuro-ophthalmology Illustrated Chapter 8 – Optic Neuropathies 5
Questions:
59. What are the fundus findings of neuroretinitis?
60. When do the retinal abnormalities of neuroretinitis appear in the course of the illness?
61. What is the most common cause of neuroretinitis?
62. How does neuroretinitis affect the risk for multiple sclerosis?
63. What is the blood supply blood to the optic nerve head?
64. What is the blood supply blood to the retrobulbar optic nerve?
65. What is the origin of the short ciliary arteries?
66. What is the origin of the long ciliary arteries?
67. Do emboli usually reach the short or long ciliary arteries?
68. What arteries supply the iris and ciliary body?
69. Is the work-up for ischemic non-arteritic optic neuropathies the same as for a retinal or a cerebral infarction?
70. How much more common is AION than PION?
Neuro-ophthalmology Illustrated Chapter 8 – Optic Neuropathies 4
Questions:
46. How is the diagnosis of neuromyelitis
47. In what setting does acute or subacute disseminated encephalomyelitis (ADEM) develop?
48. What condition may the clinical symptoms and MRI changes of acute or subacute disseminated encephalomyelitis (ADEM) mimic?
49. Is optic neuritis common in secondary and tertiary syphilis?
50. What are the typical findings of optic neuritis in secondary and tertiary syphilis?
51. What is the visual prognosis for adequately treated secondary and tertiary syphilis?
52. How is syphilitic optic neuritis treated?
53. Is syphilitic optic neuritis an uncommon cause of visual loss in patients infected with HIV?
54. What are examples of opportunistic infections invading the CNS that can produce optic neuritis?
55. Is sarcoid optic neuritis always associated with neurosarcoidosis?
56. What does the lumbar puncture often show in sarcoid optic neuritis?
57. What does the MRI typically show in sarcoid optic neuritis?
58. What kind of response to treatment is seen In most cases of sarcoid optic neuritis?
Neuro-ophthalmology Illustrated Chapter 8 – Optic Neuropathies 3
Questions:
36. In idiopathic demyelinating optic neuritis what percentage of cases have pain with eye movements?
37. In idiopathic demyelinating optic neuritis what percentage of cases is a spontaneous improvement is seen within several weeks?
38. In idiopathic demyelinating optic neuritis, what percentage of cases does visual acuity improves spontaneously to at least 20/40 at 6 months?
39. In idiopathic demyelinating optic neuritis, what is the overall risk of multiple sclerosis at 15 years?
40. In idiopathic demyelinating optic neuritis, what is the 15-year risk of multiple sclerosis if the brain MRI is normal?
41. In idiopathic demyelinating optic neuritis, what is the 15-year risk of multiple sclerosis if the brain MRI shows one T2-weighted ovoid > 3 mm in diameter, highly suggestive of multiple sclerosis?
42. In idiopathic demyelinating optic neuritis, what is the 15-year risk of multiple sclerosis if the brain MRI shows at least six T2-weighted white matter lesions suggestive of multiple sclerosis?
43. In a patient with optic neuritis and an abnormal MRI what percentage will not develop multiple sclerosis at 15 years of follow-up?
44. In idiopathic demyelinating optic neuritis, what can a lumbar puncture detect if the cause is multiple sclerosis?
45. In idiopathic demyelinating optic neuritis are oligoclonal bands in the CSF useful if the patient’s MRI has demonstrated findings consistent with multiple sclerosis?
Neuro-ophthalmology Illustrated Chapter 8 – Optic Neuropathies 2
Questions:
18. Is the onset of optic neuritis acute or subacute?
19. Is the onset of most cases of optic neuritis painful or painless?
20. Can the pain precede the vision loss in optic neuropathies?
21. Is the pain from acute optic neuropathy usually exacerbated by eye movement?
22. How long does the loss of central vision progress?
23. What 8 factors should be evaluated in a patient with a suspected recent onset of optic neuritis?
24. Under what circumstances should a lumbar puncture be done in optic neuritis?
25. Is bilateral optic neuritis is more common in children than in adults?
26. In optic neuritis, under what circumstances should an MRI of the spine with contrast be obtained?
27. In optic neuritis, under what circumstances should NMO antibodies be obtained?
28. What are the 5 categories in the classification of optic neuritis?
29. Optic neuritis is associated with what 4 demyelinating conditions?
30. What are examples of bacterial diseases associated with optic neuritis
31. What are examples of viral diseases associated with optic neuritis?
32. What are examples of parasitic diseases associated with optic neuritis? 33. What are examples of fungal diseases associated with optic neuritis?
34. What are the examples of post-vaccination optic neuritis?
35. What are the examples of inflammatory disorders associated with optic neuritis?
Neuro-ophthalmology Illustrated Chapter 8 – Optic Neuropathies 1
Questions:
1. What are optic neuropathies with an acute onset and with a normal optic nerve called?
2. What are optic neuropathies with an acute onset and with a swollen optic nerve head called?
3. After the onset of visual loss in a case of optic neuropathy, when does the optic nerve head become pale?
4. When is electrophysiologic testing is useful in acute optic neuropathies?
5. What does a painful orbital apex syndrome in a diabetic patient suggest
6. In addition to the optic nerve what structures pass through the optic canal?
7. What structures pass through the superior orbital fissure?
8. How is color vision typically affected in disease of the optic nerve?
9. How is the pupil typically affected in disease of the optic nerve?
10. How is the
11. How is the ERG typically affected in disease of the optic nerve?
12. How is the Amsler grid typically affected in disease of the optic nerve
13. How is color vision typically affected in disease of the macula?
14. How is the pupil typically affected in disease of the macula?
15. How is the
16. How is the ERG typically affected in disease of the macula?
17. How is the Amsler grid typically affected in disease of the macula?
Recommended Reading – Optical coherence tomography is a useful tool in the differentiation between true edema and pseudoedema of the optic disc.
Recommended Reading – Optical coherence tomography is a useful tool in the differentiation between true edema and pseudoedema of the optic disc.
Optical coherence tomography is a useful tool in the differentiation between true edema and pseudoedema of the optic disc.
PLoS One. 2018 Nov 29;13(11):e0208145. Carta A, Mora P, Aldigeri R, Gozzi F, Favilla S, Tedesco S, Calzetti G, Farci R, Barboni P, Bianchi-Marzoli S, Fossarello M, Gandolfi S1, Sadun AA.
Abstract
PURPOSE: To assess the usefulness of spectral-domain optical coherence tomography (SD-OCT) peripapillary retinal nerve fiber layer (RNFL) thickness measurement in discriminating early phase optic disc edema (ODE) from pseudoedema (PODE).
METHODS: Hospital-based, multicenter, cross-sectional study involving external patients referred for recent identification of “presumed ODE”. Patients underwent SD-OCT optic nerve head (ONH) RNFL thickness measurement at their first evaluation. In 155 of these, the causative etiology was subsequently ascertained and the respective eyes (one per patient) were assigned to the ODE (95 eyes) or PODE (60 eyes) group. Admission SD-OCT data were retrieved and used for the analysis. ROC curve analysis was used to calculate specificity, sensitivity and predictive value (PV) of the RNFL values.
RESULTS: The PODE group was significantly younger than the ODE group (p = 0.007). The average and any single-quadrant RNFL thickness was significantly higher in the ODE group compared with the PODE and control groups. The average and the inferior quadrant thicknesses tested the most powerful parameters to differentiate ODE from PODE. A cutoff value of ≥ 110 μm for the average area, or of ≥ 150 μm for the inferior quadrant was associated with maximal sensitivity and specificity with positive PV greater than 80%.
CONCLUSIONS: The SD-OCT evaluation of the peripapillary RNFL achieved good specificity, sensitivity and positive PV in discriminating between ODE and PODE. Despite the correct differential diagnosis between these categories still relies on a careful medical history taking and other ancillary testing, we proved the usefulness of SD-OCT RNFL measurement in supporting the diagnostic process.
Free Full Text https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6264818/
Recommended Reading – The expanding burden of idiopathic intracranial hypertension
Recommended Reading – The expanding burden of idiopathic intracranial hypertension
The expanding burden of idiopathic intracranial hypertension
Susan P. Mollan, Magda Aguiar, Felicity Evison, Emma Frew & Alexandra J. Sinclair. Eye (2018)
Free Full Text: https://www.nature.com/articles/s41433-018-0238-5
Abstract
OBJECTIVE: To quantify the hospital burden and health economic impact of idiopathic intracranial hypertension.
METHODS: Hospital Episode Statistics (HES) national data was extracted between 1st January 2002 and 31st December 2016. All those within England with a diagnosis of idiopathic intracranial hypertension were included. Those with secondary causes of raised intracranial pressure such as tumours, hydrocephalus and cerebral venous sinus thrombosis were excluded.
RESULTS: A total of 23,182 new IIH cases were diagnosed. Fifty-two percent resided in the most socially deprived areas (quintiles 1 and 2). Incidence rose between 2002 and 2016 from 2.3 to 4.7 per 100,000 in the general population. Peak incidence occurred in females aged 25 (15.2 per 100,000). 91.6% were treated medically, 7.6% had a cerebrospinal fluid diversion procedure, 0.7% underwent bariatric surgery and 0.1% had optic nerve sheath fenestration. Elective caesarean sections rates were significantly higher in IIH (16%) compared to the general population (9%), p < 0.005. Admission rates rose by 442% between 2002 and 2014, with 38% having repeated admissions in the year following diagnosis. Duration of hospital admission was 2.7 days (8.8 days for those having CSF diversion procedures). Costs rose from £9.2 to £50 million per annum over the study period with costs forecasts of £462 million per annum by 2030.
CONCLUSIONS: IIH incidence is rising (by greater than 100% over the study), highest in areas of social deprivation and mirroring obesity trends. Readmissions rates are high and growing yearly. The escalating population and financial burden of IIH has wide reaching implications for the health care system.
Composite figure.
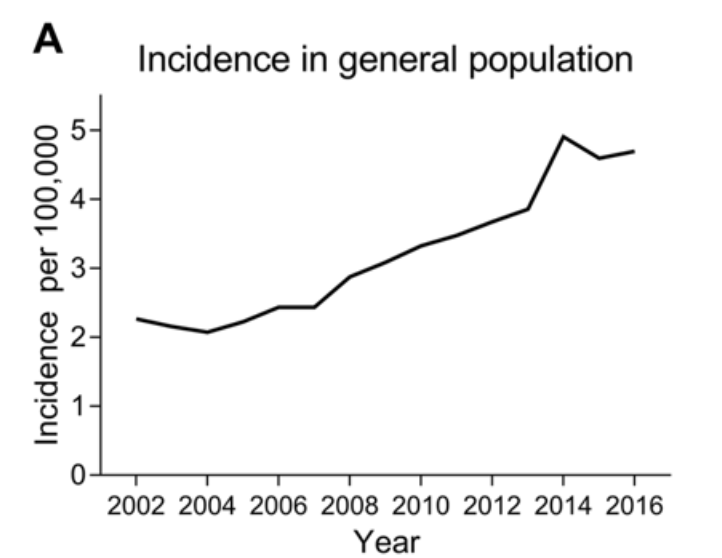
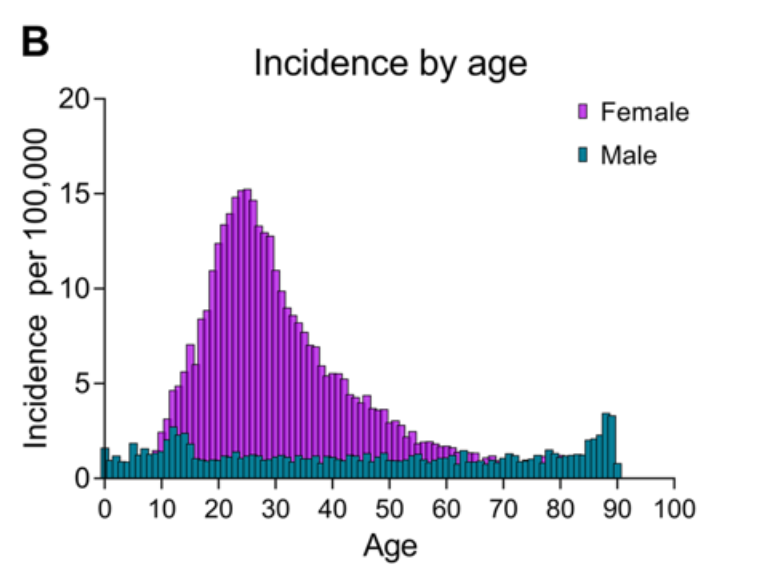
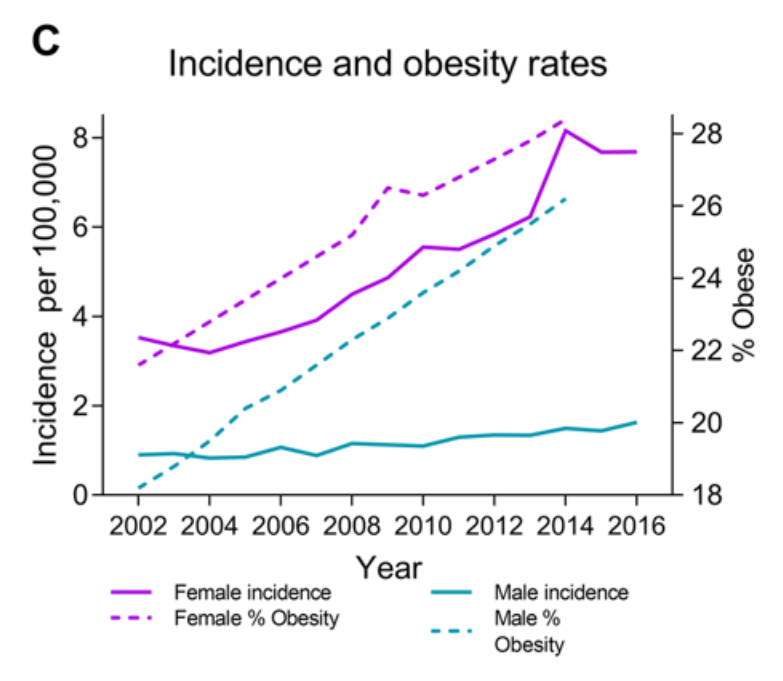
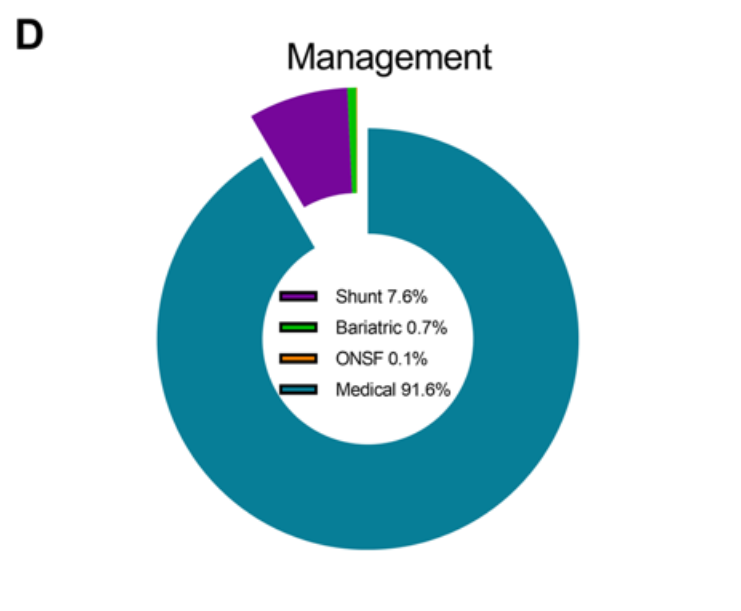
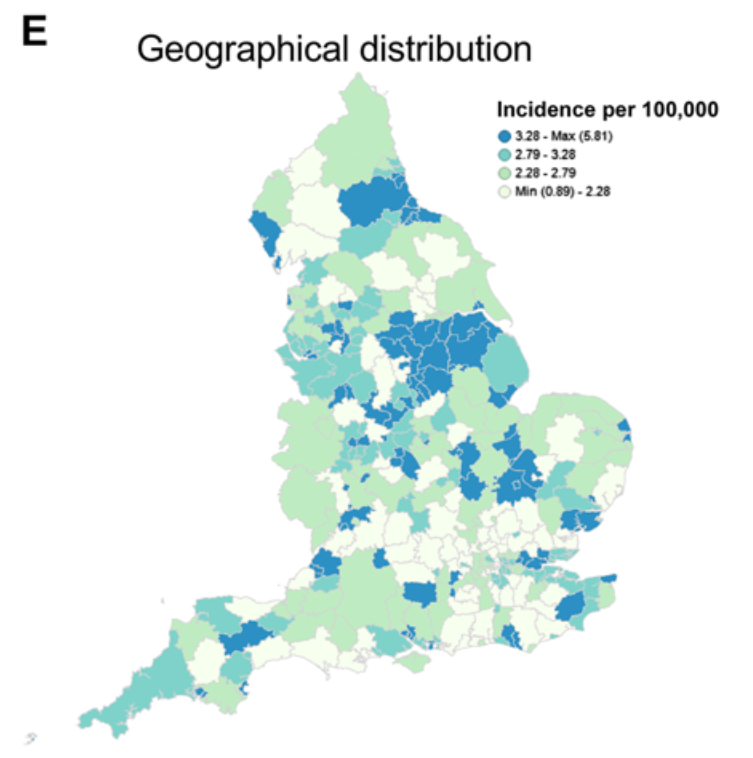
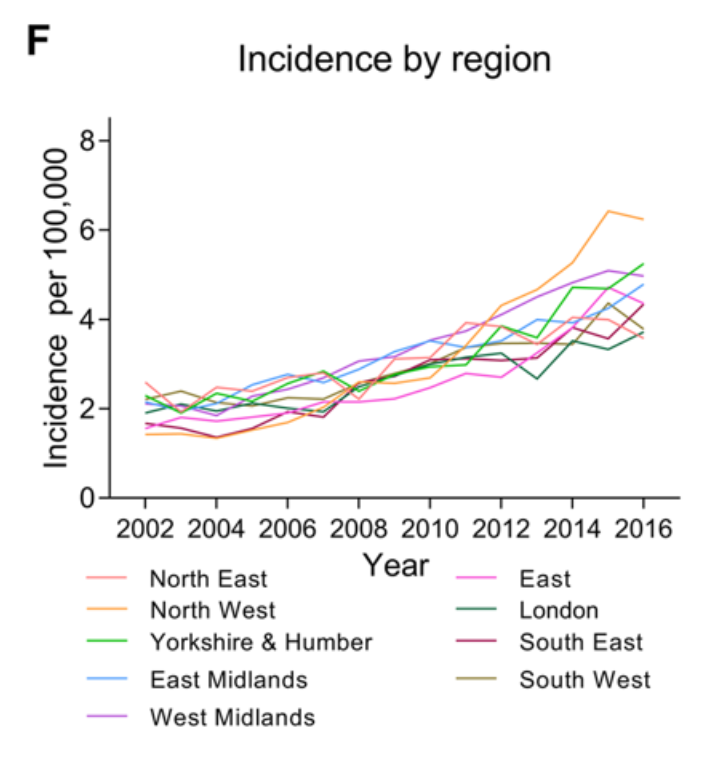
a Incidence in the general population. b Incidence by age and gender. c Annual incidence in females and males and Obesity rates (% obesity per annum (body mass index ≥ 30), age-standardized in 18 years + by gender in the United Kingdom. From World Health organisation http://apps.who.int/gho/data/node.main.A900A?lang=en Accessed 6 Oct 2017. d Management of IIH in the cohort. e Geographical distribution of diagnosed cases of IIH in England. F Distribution of cases by region per annum.
Recommended Reading – Vitamin D for the management of multiple sclerosis.
Recommended Reading – Vitamin D for the management of multiple sclerosis.
Jagannath VA1, Filippini G, Di Pietrantonj C, Asokan GV, Robak EW, Whamond L, Robinson SA.
Cochrane Database Syst Rev. 2018 Sep 24;9:CD008422.
doi: 10.1002/14651858.CD008422.pub3.
Abstract
BACKGROUND:
This review is an update of a previously published review, “Vitamin D for the management of multiple sclerosis” (published in the Cochrane Library; 2010, Issue 12). Multiple sclerosis (MS) is characterised by inflammation, demyelination, axonal or neuronal loss, and astrocytic gliosis in the central nervous system (CNS), which can result in varying levels of disability. Some studies have provided evidence showing an association of MS with low levels of vitamin D and benefit derived from its supplementation.
OBJECTIVES:
To evaluate the benefit and safety of vitamin D supplementation for reducing disease activity in people with MS.
SEARCH METHODS:
We searched the Cochrane Multiple Sclerosis and Rare Diseases of the CNS Specialized Register up to 2 October 2017 through contact with the Information Specialist with search terms relevant to this review. We included references identified from comprehensive electronic database searches and from hand searches of relevant journals and abstract books from conferences.
SELECTION CRITERIA:
We included randomised controlled trials (RCTs) and quasi-RCTs that compared vitamin D versus placebo, routine care, or low doses of vitamin D in patients with MS. Vitamin D was administered as monotherapy or in combination with calcium. Concomitant interventions were allowed if they were used equally in all trial intervention groups.
DATA COLLECTION AND ANALYSIS:
Two review authors independently extracted data and assessed the methodological quality of studies, while another review author sorted any disagreements. We expressed treatment effects as mean differences (MDs) for continuous outcomes (Expanded Disability Status Scale and number of magnetic resonance imaging (MRI) gadolinium-enhancing T1 lesions), as standardised MDs for health-related quality of life, as rate differences for annualised relapse rates, and as risk differences (RDs) for serious adverse events and minor adverse events, together with 95% confidence intervals (CIs).
MAIN RESULTS:
We identified 12 RCTs enrolling 933 participants with MS; 464 were randomised to the vitamin D group, and 469 to the comparator group. Eleven trials tested vitamin D₃, and one trial tested vitamin D₂. Vitamin D₃ had no effect on the annualised relapse rate at 52 weeks’ follow-up (rate difference -0.05, 95% CI -0.17 to 0.07; I² = 38%; five trials; 417 participants; very low-quality evidence according to the GRADE instrument); on the Expanded Disability Status Scale at 52 weeks’ follow-up (MD -0.25, 95% CI -0.61 to 0.10; I² = 35%; five trials; 221 participants; very low-quality evidence according to GRADE); and on MRI gadolinium-enhancing T1 lesions at 52 weeks’ follow-up (MD 0.02, 95% CI -0.45 to 0.48; I² = 12%; two trials; 256 participants; very low-quality evidence according to GRADE). Vitamin D₃ did not increase the risk of serious adverse effects within a range of 26 to 52 weeks’ follow-up (RD 0.01, 95% CI -0.03 to 0.04; I² = 35%; eight trials; 621 participants; low-quality evidence according to GRADE) or minor adverse effects within a range of 26 to 96 weeks’ follow-up (RD 0.02, 95% CI -0.02 to 0.06; I² = 20%; eight trials; 701 participants; low-quality evidence according to GRADE). Three studies reported health-related quality of life (HRQOL) using different HRQOL scales. One study reported that vitamin D improved ratings on the psychological and social components of the HRQOL scale but had no effects on the physical components. The other two studies found no effect of vitamin D on HRQOL. Two studies reported fatigue using different scales. One study (158 participants) reported that vitamin D₃ reduced fatigue compared with placebo at 26 weeks’ follow-up. The other study (71 participants) found no effect on fatigue at 96 weeks’ follow-up. Seven studies reported on cytokine levels, four on T-lymphocyte proliferation, and one on matrix metalloproteinase levels, with no consistent pattern of change in these immunological outcomes. The randomised trials included in this review provided no data on time to first treated relapse, number of participants requiring hospitalisation owing to progression of the disease, proportion of participants who remained relapse-free, cognitive function, or psychological symptoms.
AUTHORS’ CONCLUSIONS:
To date, very low-quality evidence suggests no benefit of vitamin D for patient-important outcomes among people with MS. Vitamin D appears to have no effect on recurrence of relapse, worsening of disability measured by the Expanded Disability Status Scale (EDSS), and MRI lesions. Effects on health-related quality of life and fatigue are unclear. Vitamin D₃ at the doses and treatment durations used in the included trials appears to be safe, although available data are limited. Seven ongoing studies will likely provide further evidence that can be included in a future update of this review.
Update of Vitamin D for the management of multiple sclerosis. [Cochrane Database Syst Rev. 2010]
Full Text https://drive.google.com/open?id=1_ESVaPi-Rea_BzZ7E-EbJp-y7GR_6ZMU
Neuro-ophthalmology questions of the week: NOI20-Conditions Commonly Encountered in Neuro-ophthalmology 3
Questions:
25. Multiple sclerosis is more common in:
a. Men or Women,
b. African-Americans, Caucasians, or Hispanics?
26. What is Lhermitte sign and is it a classic finding in Multiple sclerosis?
27. What are common eye manifestations of multiple sclerosis?
28. What is the 15-year risk of multiple sclerosis after an initial episode of optic neuritis:
a. Overall,
b. With no MRI lesions,
c. With 1 or more lesions on MRI?
29. How common is mild-to-severe eye pain in optic neuritis?
30. What are the characteristics of Neuromyelitis Optica (Devic disease)?
31. What treatment is useful for Neuromyelitis Optica?