Questions:
1. What are optic neuropathies with an acute onset and with a normal optic nerve called?
2. What are optic neuropathies with an acute onset and with a swollen optic nerve head called?
3. After the onset of visual loss in a case of optic neuropathy, when does the optic nerve head become pale?
4. When is electrophysiologic testing is useful in acute optic neuropathies?
5. What does a painful orbital apex syndrome in a diabetic patient suggest
6. In addition to the optic nerve what structures pass through the optic canal?
7. What structures pass through the superior orbital fissure?
8. How is color vision typically affected in disease of the optic nerve?
9. How is the pupil typically affected in disease of the optic nerve?
10. How is the
11. How is the ERG typically affected in disease of the optic nerve?
12. How is the Amsler grid typically affected in disease of the optic nerve
13. How is color vision typically affected in disease of the macula?
14. How is the pupil typically affected in disease of the macula?
15. How is the
16. How is the ERG typically affected in disease of the macula?
17. How is the Amsler grid typically affected in disease of the macula?
___________________________________________
Questions with answers:
1. What are optic neuropathies with an acute onset and with a normal optic nerve called?
Posterior or retrobulbar optic neuropathies
2. What are optic neuropathies with an acute onset and with a swollen optic nerve head called?
Anterior optic neuropathies
3. After the onset of visual loss from optic neuropathy, when does the optic nerve head become pale?
In almost all cases, the optic nerve becomes pale 4 to 6 weeks after the onset of visual loss, even when vision recovers.
4. When is electrophysiologic testing is useful in acute optic neuropathies?
Visual evoked responses and electroretinograms are useful when the diagnosis is unclear (e. g. , in cases with bilateral visual loss and no RAPD and when there is
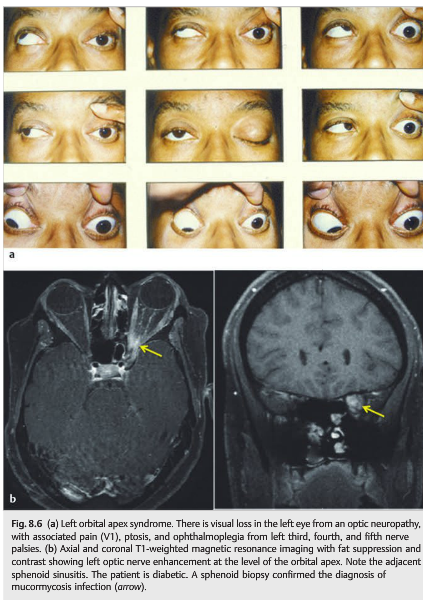
5. What does a painful orbital apex syndrome in a diabetic patient suggest?
It is highly suggestive of mucormycosis infection.
6. In addition to the optic nerve what structures pass through the optic canal?
The ophthalmic artery.
7. What structures pass through the superior orbital fissure?
The superior ophthalmic vein, cranial nerves III (superior and inferior branches), IV, V1 (lacrimal, frontal, and nasociliary nerves), VI and sympathetic fibers from cavernous plexus.
8. How is color vision typically affected in disease of the optic nerve?
Color vision is very reduced.
9. How is the pupil typically affected in disease of the optic nerve?
There is a reduced response to light producing a RAPD if the optic neuropathy is unilateral or asymmetric.
10. How is the photostress test recovery typically affected in disease of the optic nerve?
It is not affected, there is normal recovery within 30 seconds (returns to within one line of the best corrected visual acuity after the patient views a bright light held a few centimeters from the eye for 10 seconds).
11. How is the ERG typically affected in disease of the optic nerve?
It is not affected
12. How is the Amsler grid typically affected in disease of the optic nerve?
Scotoma
13. How is color vision typically affected in disease of the macula?
Typically color vision is mildly reduced.
14. How is the pupil typically affected in disease of the macula?
No RAPD, unless the entire or macula is affected.
15. How is the photostress test recovery typically affected in disease of the macula?
Delayed recovery, not within 30 seconds.
16. How is the ERG typically affected in disease of the macula?
Full-field ERG often normal. Multifocal ERG is usually abnormal.
17. How is the Amsler grid typically affected in disease of the macula?
Metamorphopsia
___________________________________________
From: Clinical Pathways in Neuro-ophthalmology 2nd Edition – Lee & Brazis. Thieme

___________________________________________
The information below is
8 Optic Neuropathies
Disorders of the optic nerve are called optic neuropathies. Optic neuropathies associated acutely with a normal optic nerve are referred to as posterior or retrobulbar optic neuropathies. Those with optic nerve head swelling are anterior optic neuropathies.



8.1 Diagnosis
The diagnosis of optic neuropathy is based on clinical examination, checking for the following:
● Visual loss
● Impaired color vision
● Abnormal visual field
● Relative afferent pupillary defect (RAPD) in all unilateral or asymmetric optic neuropathies (▶Fig. 8.3)
● Optic nerve head appearance
○ Acutely: normal or swollen
○ Late (after 4–6 weeks): pale


Electrophysiologic testing is most often unnecessary. However, visual evoked responses and electroretinography are useful when the diagnosis is unclear (e.g., in cases with bilateral visual loss and no RAPD and when there is
8.1.1 Localization of the Lesion
The optic nerve may be affected in the orbit, at the level of the optic canal, or in its intracranial portion. In the orbit, the optic neuropathy may be isolated. The presence of associated symptoms or signs such as diplopia, ptosis, and proptosis suggests a process involving more than just the optic nerve, such as inflammation, infection, or neoplasm (▶Fig. 8.5 and ▶Fig. 8.6).

Pearls
A painful orbital apex syndrome in a diabetic patient is highly suggestive of mucormycosis infection.


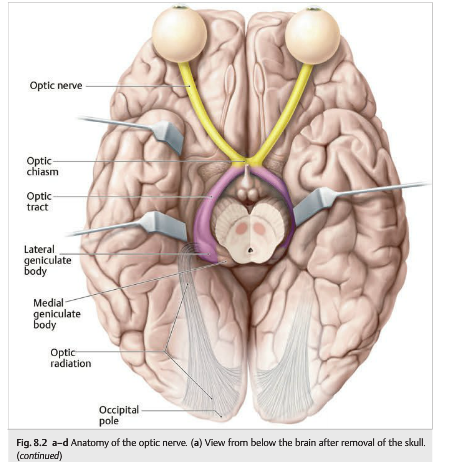
Neurovascular structures enter and exit the orbit through the optic canal and the superior orbital fissure. In the optic canal, the optic nerve exits the orbit, and the ophthalmic artery enters the orbit. In the superior orbital fissure, the superior ophthalmic vein exits the orbit, and cranial nerves III (superior and inferior branches), IV, V1(lacrimal, frontal, and nasociliary nerves), and VI enter the orbit (▶Fig. 8.7). An optic neuropathy may result from a lesion involving the intracranial portion of the optic nerve. When the lesion is close to the optic chiasm, visual field testing demonstrates a junctional scotoma (▶Fig. 8.8).

8.2 Types of Optic Neuropathies (▶Table 8.1)
The following lists the main types of optic neuropathies, with subcategories:
● Inflammatory (optic neuritis)
○ Idiopathic demyelinating optic neuritis (associated with multiple sclerosis)
○ Neuromyelitis
○ Acute disseminated encephalomyelitis
○ Systemic infections
○ Systemic inflammatory diseases (e.g., sarcoidosis)
● Vascular (ischemic optic neuropathy)
○ Anterior/posterior
○ Arteritic/nonarteritic
● Compressive/infiltrative
○ Neoplastic
○ Non-neoplastic
● Hereditary
● Toxic/nutritional
● Traumatic
● Raised intracranial pressure (papilledema)
● Glaucomatous
● Anomalous optic nerve
○ Congenitally anomalous
○ Drusen
Optic neuropathies and maculopathies have overlapping presentations. Both cause central visual loss and dyschromatopsia. Many chronic maculopathies are associated with mild optic nerve pallor. When the macula appears normal, it may be difficult to differentiate an optic neuropathy from a maculopathy (▶Table 8.2). Autofluorescence imaging of the macula and spectral optical coherence tomography (OCT) are very helpful in distinguishing optic neuropathies from maculopathies when the macula appears normal on funduscopic examination.

8.3 Patient Evaluation
The following clinical characteristics are particularly helpful in determining the mechanism of the optic neuropathy:
● Mode of onset of visual loss
○ Acute (ischemic and inflammatory neuropathies)
○ Progressive (compressive or toxic optic neuropathies)
● Color vision (often relatively spared in ischemic optic neuropathies and usually very abnormal ● The presence of pain with eye movements (highly suggestive of an inflammatory in inflammatory optic neuropathies)
mechanism)
● Funduscopic appearance (variable in inflammatory optic neuropathies, reveals a swollen optic nerve in all cases of anterior ischemic optic neuropathy, and shows sometimes cupped optic nerve in compressive and hereditary optic neuropathies)
● Associated retinal changes in
Evaluating the patient with suspected optic neuropathy includes the following:
1. Confirm the diagnosis of optic neuropathy by clinical examination.
2. Look for associated symptoms and signs.
3. Try to localize the optic nerve lesion (anterior, posterior in the orbit, orbital apex, or intracranial).
4. Determine the presumed etiologic diagnosis.
5. Obtain ancillary testing, such as imaging and laboratory workup, to confirm the diagnosis prior to initiating treatment.
Recommended tests include the following:
● Magnetic resonance imaging (MRI) of the brain and orbits with gadolinium (orbital images should be with fat suppression)
● Blood tests
○ Blood tests will vary, based on the presumed diagnosis.
○ Helpful tests include those for syphilis, sarcoidosis (angiotensin-converting enzyme[ACE]), cat scratch disease (Bartonella antibodies), Lyme disease, human immunodeficiency virus (HIV), inflammatory biologic syndrome (complete blood count[CBC], C-reactive protein [CRP], and erythrocyte sedimentation rate [ESR]), autoantibodies for autoimmune diseases (antinuclear antibodies [ANAs] and anti-neutrophil cytoplasmic antibodies [ANCAs]), and vitamin B12 and folate (bilateral and progressive painless optic neuropathies), as well as genetic testing for Leber Hereditary optic neuropathy (severe unilateral or bilateral optic neuropathies) and for dominant optic atrophy (bilateral and progressive painless optic neuropathies).
● Cerebrospinal fluid (CSF) (lumbar puncture)
○ Helpful in cases of bilateral optic neuropathies, or when an infectious, systemic inflammatory, or neoplastic cause is suspected.
Reference:
1. Clinical Pathways in Neuro-ophthalmology 2nd Edition. Lee A and Brazis P. 2003. Thieme
2. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.