Questions:
59. What are the fundus findings of neuroretinitis?
60. When do the retinal abnormalities of neuroretinitis appear in the course of the illness?
61. What is the most common cause of neuroretinitis?
62. How does neuroretinitis affect the risk for multiple sclerosis?
63. What is the blood supply blood to the optic nerve head?
64. What is the blood supply blood to the retrobulbar optic nerve?
65. What is the origin of the short ciliary arteries?
66. What is the origin of the long ciliary arteries?
67. Do emboli usually reach the short or long ciliary arteries?
68. What arteries supply the iris and ciliary body?
69. Is the work-up for ischemic non-arteritic optic neuropathies the same as for a retinal or a cerebral infarction?
70. How much more common is AION than PION?
____________________________________________________
Questions with answers:
59. What are the fundus findings of neuroretinitis?
Neuroretinitis is characterized by optic disk swelling associated with a macular star figure composed of lipid.
60. When do the retinal abnormalities of neuroretinitis appear in the course of the illness?
The retinal abnormalities typically appear days to weeks after the onset of visual loss.
61. What is the most common cause of neuroretinitis?
This form of optic neuritis is not caused by demyelination and occurs most often in the setting of cat scratch disease or in association with other systemic infectious diseases, such as Lyme disease and syphilis, as well as with sarcoidosis.
62. How does neuroretinitis affect the risk for multiple sclerosis
Neuroretinitis does not increase the subsequent risk for the development of multiple sclerosis
63. What is the blood supply blood to the optic nerve head?
The prelaminar (inside the eye relative to the lamina cribrosa) optic nerve is supplied by collaterals from the choroidal and retinal circulations. The laminar zone is supplied by branches from the short posterior ciliary and pial arteries. The post laminar zone is supplied by the pial arteries.
64. What is the blood supply blood to the retrobulbar optic nerve?
The peripheral centripetal vascular system of the optic nerve is formed by the pial vascular plexus, supplied by multiple small collateral arteries usually arising directly from the ophthalmic artery.
65. What is the origin of the short ciliary arteries?
The ophthalmic artery.
66. What is the origin of the long ciliary arteries?
The ophthalmic artery.
67. Do emboli usually reach the short or long ciliary arteries?
No, these are small arteries that may be affected by several local disorders, such as atherosclerosis and vasculitis. Emboli do not usually reach these arteries.
68. What arteries supply the iris and ciliary body?
The iris and ciliary body are supplied by the anterior ciliary arteries, the long posterior ciliary arteries and anastomotic connections from the anterior choroid.
69. Is the work-up for ischemic non-arteritic optic neuropathies the same as for a retinal or a cerebral infarction?
No. Although ischemic optic neuropathies are considered the equivalent of a “stroke of the optic nerve,” the causes and mechanisms of ischemic optic neuropathies are different than a retinal artery occlusion or a cerebral infarction which require an emergent stroke work up. Nonarteritic AION is not an embolic disorder. Evaluation of the internal carotid artery is not indicated in isolated, typical AION. There is no definite increased risk of cerebrovascular disease in the population of patients with AION, but vascular risk factors are common and should be controlled.
70. How much more common is AION than PION?
90%
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
Neuroretinitis
Neuroretinitis associated inflammation of the optic nerve head with retinal lesions. It is characterized ophthalmoscopically by optic disc swelling associated with a macular star figure composed of lipid. The retinal abnormalities typically appear days to weeks after the onset of visual loss. This form of optic neuritis is not caused by demyelination and occurs most often in the setting of cat scratch disease or in association with other systemic infectious diseases, such as Lyme disease and syphilis, as well as with sarcoidosis. These patients are not at subsequent risk for the development of multiple sclerosis (▶Fig. 8.14 and ▶Fig. 8.15).


Optic Neuritis in Children
As in adults, optic neuritis is often the first sign of multiple sclerosis in children. Infectious causes are also common. Bilateral optic neuritis is also more common in children than in adults. Children with acute optic neuritis are usually evaluated and treated similarly to adults.
8.5 Ischemic Optic Neuropathy
Ischemic optic neuropathies are the most common acute optic neuropathies in patients over 50 years of age; they can rarely occur in younger patients, in whom they must be differentiated from other causes of optic neuropathies such as optic neuritis. The term ischemic optic neuropathy is used to refer to all presumed ischemic causes of optic neuropathy.
8.5.1 Clinical Anatomy
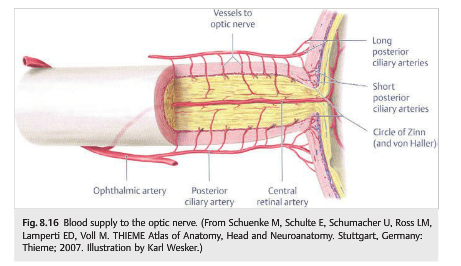

The posterior ciliary arteries provide the blood supply to the optic nerve (short posterior ciliary arteries to the optic nerve head and long posterior ciliary arteries to the retrobulbar optic nerve). They originate from the ophthalmic artery. These are small arteries that may be affected by several local disorders, such as atherosclerosis and vasculitis. Emboli do not usually reach these arteries (▶Fig. 8.16).
Because of the anatomy of the posterior ciliary arteries, optic nerve ischemia often results in superior (more often) or inferior segmental optic nerve atrophy. There is pallor affecting only the superior or inferior half of the optic nerve. This explains why altitudinal defects are common with ischemic optic neuropathies. Superior segmental optic atrophy results in an inferior altitudinal defect (▶Fig. 8.17).
Pearls
Although ischemic optic neuropathies are considered the equivalent of a “stroke of the optic nerve,” they cannot be directly compared with cerebral infarctions. The causes and mechanisms of ischemic optic neuropathies are different, and the workup of a patient with an ischemic optic neuropathy is not the same as that for patients with retinal or cerebral infarction.
8.5.2 Classification
Ischemic optic neuropathies include anterior ischemic optic neuropathy (AION), which is always associated with disc edema, and posterior ischemic optic neuropathy (PION), when the optic nerve appears normal acutely. AION is much more common than PION, accounting for 90% of cases of optic nerve ischemia.
Ischemic optic neuropathies are categorized as nonarteritic ischemic optic neuropathy and arteritic ischemic optic neuropathy (usually in the setting of giant cell arteritis). Patients with giant cell arteritis and ischemic optic neuropathy are in danger of catastrophic, irreversible, bilateral total blindness that may be prevented by prompt treatment with corticosteroid therapy.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.