Questions:
46. How is the diagnosis of neuromyelitis
47. In what setting does acute or subacute disseminated encephalomyelitis (ADEM) develop?
48. What condition may the clinical symptoms and MRI changes of acute or subacute disseminated encephalomyelitis (ADEM) mimic?
49. Is optic neuritis common in secondary and tertiary syphilis?
50. What are the typical findings of optic neuritis in secondary and tertiary syphilis?
51. What is the visual prognosis for adequately treated secondary and tertiary syphilis?
52. How is syphilitic optic neuritis treated?
53. Is syphilitic optic neuritis an uncommon cause of visual loss in patients infected with HIV?
54. What are examples of opportunistic infections invading the CNS that can produce optic neuritis?
55. Is sarcoid optic neuritis always associated with neurosarcoidosis?
56. What does the lumbar puncture often show in sarcoid optic neuritis?
57. What does the MRI typically show in sarcoid optic neuritis?
58. What kind of response to treatment is seen In most cases of sarcoid optic neuritis?
____________________________________________________
Questions with answers:
46. How is the diagnosis of neuromyelitis optica (NMO), Devic disease, made?
In the presence of optic neuritis, NMO is diagnosed with an abnormal cervical spine MRI (long T2-weighted hypersignal over more than three segments) and a brain MRI that is typically normal or shows T2-weighted hypersignals not typical of multiple sclerosis (i.e. not involving the periventricular region and not scattered in the white matter). There are also positive NMO immunoglobulin (IgG) antibodies, Aquaporin 4 Protein (AQP4).
47. In what setting does acute or subacute disseminated encephalomyelitis (ADEM) develop?
ADEM usually occurs during or after a febrile illness or immunization. It is an immune-mediated inflammatory demyelinating condition that mostly affects the white matter of the brain and spinal cord. The disorder manifests as an acute-onset encephalopathy associated with multifocal neurologic deficits and is typically self-limiting. It is particularly common in children, but it may occur at any age.
48. What condition may the clinical symptoms and MRI changes of acute or subacute disseminated encephalomyelitis (ADEM) mimic?
The clinical symptoms and MRI changes may mimic multiple sclerosis; however, unlike multiple sclerosis, which is a relapsing-remitting disorder, patients usually have only one episode of ADEM. Unilateral or bilateral optic neuritis (often with disk edema) may develop during the course of ADEM.
49. Is optic neuritis common in secondary and tertiary syphilis?
Yes, it is usually associated with lymphocytic meningitis and is a sign of neurosyphilis.
50. What are the typical findings of optic neuritis in secondary and tertiary syphilis?
Optic neuritis is common in secondary and tertiary syphilis. It is usually associated with lymphocytic meningitis and is a sign of neurosyphilis. Raised intracranial pressure with papilledema is common with syphilitic lymphocytic meningitis.
51. What is the visual prognosis for adequately treated secondary and tertiary syphilis?
Usually good.
52. How is syphilitic optic neuritis treated?
It is treated like neurosyphilis.
53. Is syphilitic optic neuritis an uncommon cause of visual loss in patients infected with HIV?
Syphilitic optic neuritis is not an uncommon cause of visual loss in patients infected with HIV and is the most common cause of optic neuritis in patients with HIV.
54. What are examples of opportunistic infections invading the CNS that can produce optic neuritis?
Most opportunistic infections invading the CNS can produce optic neuritis. Cytomegalovirus, toxoplasmosis, and
55. Is sarcoid optic neuritis always associated with neurosarcoidosis?
Not always, sarcoid optic neuritis may be isolated, or it may develop in a patient with neurosarcoidosis.
56. What does the lumbar puncture often show in sarcoid optic neuritis?
The lumbar puncture often shows lymphocytic meningitis.
57. What does the MRI typically show in sarcoid optic neuritis?
The MRI typically demonstrates intense gadolinium enhancement of the affected optic nerve and sometimes there is a meningeal enhancement.
58. What kind of response to treatment is seen In most cases of sarcoid optic neuritis?
Typically the optic neuropathy responds well to corticosteroids and may be steroid-dependent, requiring long-term treatment with an immunosuppressive agent.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
8.4.6 Neuromyelitis Optica (Devic Disease)
NMO, also known as Devic disease, is the association of acute or subacute severe visual loss in one or both eyes caused by acute optic neuritis. Transverse myelopathy precedes or follows visual loss. NMO is diagnosed with an abnormal cervical spine MRI scan (long T2-weighted
The prognosis is usually poor, with permanent, severe visual loss and paraplegia.
Treatment usually consists of high-dose intravenous steroids followed by a slow taper of oral prednisone and long-term immunosuppressive therapy. Plasmapheresis is sometimes performed in cases with acute symptoms (▶Fig. 8.10).

Neuromyelitis optica (NMO) is an inflammatory CNS syndrome distinct from multiple sclerosis (MS) that is associated with serum aquaporin-4 immunoglobulin G antibodies (AQP4-IgG). Prior NMO diagnostic criteria required optic nerve and spinal cord involvement but more restricted or more extensive CNS involvement may occur. The International Panel for NMO Diagnosis (IPND) was convened to develop revised diagnostic criteria using systematic literature reviews and electronic surveys to facilitate consensus. The new nomenclature defines the unifying term NMO spectrum disorders (NMOSD), which is stratified further by serologic testing (NMOSD with or without AQP4-IgG). The core clinical characteristics required for patients with NMOSD with AQP4-IgG include clinical syndromes or MRI findings related to optic nerve, spinal cord, area postrema, other brainstem, diencephalic, or cerebral presentations. More stringent clinical criteria, with additional neuroimaging findings, are required for diagnosis of NMOSD without AQP4-IgG or when serologic testing is unavailable. The IPND also proposed validation strategies and achieved consensus on pediatric NMOSD diagnosis and the concepts of monophasic NMOSD and opticospinal MS.
8.4.7 Acute Disseminated Encephalomyelitis
ADEM or subacute encephalomyelitis occurs during the course of various infections, most often as a post infectious or autoimmune response. It is particularly common in children, but it may occur at any age.
The clinical symptoms and MRI changes may mimic multiple sclerosis; however, unlike multiple sclerosis, which is a relapsing-remitting disorder, patients usually have only one episode of ADEM. Unilateral or bilateral optic neuritis (often with disc edema)may develop during the course of ADEM.
8.4.8 Other Causes of Optic Neuritis
Less commonly, inflammatory optic neuritis is not associated with a primary demyelinating process in the optic nerve or the central nervous system (CNS). Instead, the condition develops in the setting, or as the presenting manifestation, of a systemic infection or a systemic inflammatory disease.
Systemic symptoms and signs, patients’ characteristics, and associated ocular findings such as neuroretinitis should direct the subsequent workup.
Syphilitic Optic Neuritis

Optic neuritis is common in secondary and tertiary syphilis. It is usually associated with lymphocytic meningitis and is a sign of neurosyphilis. Raised intracranial pressure with papilledema is common with syphilitic lymphocytic meningitis. Testing for syphilis (rapid plasma reagin [RPR] and fluorescent treponemal antibody absorption [FTA-ABS]) should be considered in patients with optic neuritis. When blood tests are positive, a lumbar puncture (with opening pressure, CSF analysis, and Venereal Disease Research Laboratories [VDRL] testing) and HIV testing are mandatory. Syphilitic optic neuritis is treated like neurosyphilis. The visual prognosis is usually good (▶Fig. 8.11).

Optic Neuritis in Patients with HIV
Optic neuritis is a not uncommon cause of visual loss in patients infected with HIV (see Chapter 20). Syphilis is the most common cause of optic neuritis in patients with HIV. Most opportunistic infections invading the CNS can produce an optic neuritis. Infections by cytomegalovirus, toxoplasmosis, and cryptococcus are the most classic causes. A lumbar puncture should always be performed, and CSF should be evaluated for all causes of infections and malignancies (e.g., lymphoma) common in patients with HIV(▶Fig. 8.12).
Sarcoid Optic Neuritis
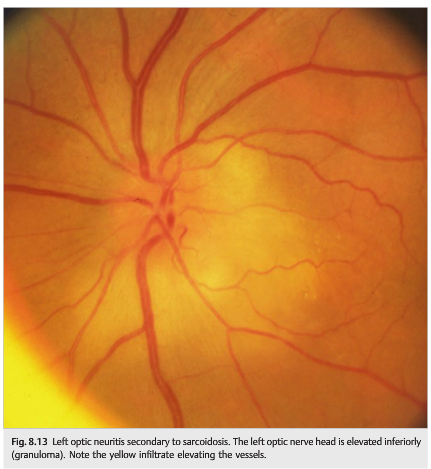
Sarcoid optic neuritis may be isolated, or it may develop in a patient with neurosarcoidosis (see discussion in Chapter 20). The lumbar puncture often shows abnormal CSF (lymphocytic meningitis), and the MRI scan typically demonstrates intense gadolinium enhancement of the affected optic nerve. There is sometimes associated meningeal enhancement. Workup (general examination, ACE level, chest radiograph, chest computed tomography [CT], gallium scan, or fluorodeoxyglucose positron-emission tomography [FDG-PET] scan) may suggest systemic sarcoidosis. Biopsy of a lesion (usually skin lesion, lymph node, pulmonary lesion, or lacrimal gland) confirms the diagnosis of sarcoidosis. In sarcoidosis, the optic neuritis may result from lymphocytic meningitis present in neurosarcoidosis. Uni- or bilateral optic nerve edema may be present if there is raised intracranial pressure. Optic neuritis may also result from granulomatous infiltration of the optic nerve head associated with elevation of the optic nerve. Retinal lesions (infiltrates, vasculitis) and vitreous cells are common in this setting. Another cause is granulomatous infiltration of the intracranial portion of the optic nerve and the chiasm.
In most cases, the optic neuropathy responds well to corticosteroids and may be steroid-dependent, requiring long-term treatment with an immunosuppressive agent (▶Fig. 8.13).
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.