Questions:
71. What should the findings of AION in the absence of a small crowded optic nerve head with a small cup-to-disk ratio suggest?
72. Which is more likely to have pain, nonarteritic AION or Arteritic AION
73. If the reduction of visual acuity is small in nonarteritic AION, how is color vision likely to be affected?
74. What kind of process is believed to be present in diabetic papillopathy?
75. How is diabetic papillopathy distinguished from typical nonarteritic AION?
76. Is nonarteritic AION associated with ipsilateral internal carotid artery stenosis?
77. What are 9 risk factors for nonarteritic AION?
78. Should the internal carotid arteries be evaluated in nonarteritic AION?
79. Is there an increased risk of cerebrovascular disease in the population of patients with AION?
80. Does the presence of optic nerve head drusen or papilledema increase the risk of nonarteritic AION?
81. What medication may induce an optic neuropathy that mimics nonarteritic AION?
82. Is there a proven treatment for nonarteritic AION?
83. What conditions are associated with nonarteritic PION?
84. How is nonarteritic PION diagnosed?
____________________________________________________
Questions with answers:
71. What should the findings of AION in the absence of a small crowded optic nerve head with a small cup-to-disk ratio suggest?
The absence of a disk-at-risk in a patient with AION should suggest giant cell arteritis or another underlying disorder. In a patient with suspected ischemic optic neuropathy, the first step should always be to consider giant cell arteritis.
72. Which is more likely to have pain, nonarteritic AION or Arteritic AION
Arteritic AION.
73. If the reduction of visual acuity is small in nonarteritic AION, how is color vision likely to be affected?
In nonarteritic AION color vision is commonly spared if acuity is good.
74. What kind of process is believed to be present in diabetic papillopathy?
Diabetic papillopathy is believed to be an atypical form of AION that usually occurs in young patients with insulin-dependent diabetes.
75. How is diabetic papillopathy distinguished from typical nonarteritic AION?
It is distinguished from typical nonarteritic AION by the slight degree (or even absence) of visual loss, the frequency of bilateral involvement (50%), the long duration of disk edema, and the good visual outcome.
76. Is nonarteritic AION associated with ipsilateral internal carotid artery stenosis?
As a disease of the small vessels, nonarteritic AION is not associated with ipsilateral internal carotid artery stenosis, and embolic AION is extremely rare.
77. What are 9 risk factors for nonarteritic AION?
1. Small, crowded disk (disk-at-risk)
2. Other abnormalities localized to the disk: (Optic nerve head drusen, an anomalous disk
3. Severe papilledema
4. Severe hypotension (Operative, Systemic massive hemorrhage, Cardiac arrest, Renal dialysis)
5. Anemia
6. Hypercoagulable disorders
7. Radiation optic neuropathy
8. Acute intraocular hypertension (during ocular surgery, after an intravitreal injection of steroids, or during an attack of angle-closure glaucoma)
9. Vascular risk factors for atherosclerosis (hypertension, diabetes, hyperlipidemia)
78. Should the internal carotid arteries be evaluated in nonarteritic AION?
Nonarteritic AION is not an embolic disorder. Evaluation of the internal carotid arteries is not indicated in isolated, typical AION.
79. Is there an increased risk of cerebrovascular disease in the population of patients with AION?
There is no definite increased risk of cerebrovascular disease in the population of patients with AION, but vascular risk factors are common and should be controlled.
80. Does the presence of optic nerve head drusen or papilledema increase the risk of nonarteritic AION?
Yes, AION may occur in a patient with optic nerve head drusen or papilledema. The drusen or the papilledema makes the optic nerve head more crowded and may “choke” the optic nerve head, which becomes ischemic.
81. What medication may induce an optic neuropathy that mimics nonarteritic AION?
Amiodarone may induce an optic neuropathy mimicking nonarteritic AION.
82. Is there a proven treatment for nonarteritic AION?
There is no established treatment for nonarteritic AION. The clinician’s primary role is to exclude giant cell arteritis, control vascular risk factors, treat anemia, and prevent hypotension (e. g. , in the setting of dialysis).
83. What conditions are associated with nonarteritic PION?
Nonarteritic PION is extremely rare and may occur during lengthy spine or cardiac surgery and in patients with acute systemic hypotension.
84. How is nonarteritic PION diagnosed?
It is a diagnosis of exclusion made only after compression of the posterior optic nerve is ruled out by a good quality MRI of the orbits with contrast and fat suppression, along with an extensive systemic workup looking for an underlying systemic inflammatory disorder. Non-operative PION in patients older than age 50 is usually indicative of giant cell arteritis.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
Pearls
Nonarteritic AION typically occurs in the setting of a disc-at-risk (small crowded optic nerve with a small cup-to-disc ratio) (▶Fig. 8.18). The absence of a disc-at-risk in a patient with AION should suggest giant cell arteritis or another underlying disorder.
In a patient with suspected ischemic optic neuropathy, the first step should always be to consider giant cell arteritis.

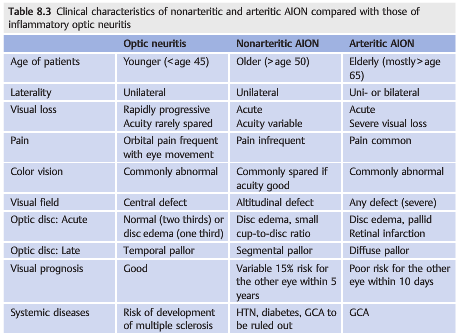
It is essential to correctly diagnose patients with ischemic optic neuropathies. Indeed, inflammatory optic neuritis is often over diagnosed in patients with acute optic neuropathy, especially in patients younger than 50. A brain MRI scan is usually obtained in these patients, who may be found to have one hyperintensity on the T2-weighted images. This inappropriately prompts a diagnosis of optic neuritis and presumed multiple sclerosis with dramatic consequences for the patient’s life and treatment. In addition, when ischemic optic neuropathy is missed, then giant cell arteritis may also be overlooked (▶Table 8.3).

8.5.3 Nonarteritic Anterior Ischemic Optic Neuropathy Characteristics
Nonarteritic AION (▶Fig. 8.19) is most common in Caucasians older than age 50.
It is characterized by acute, painless monocular loss of vision that may progress over several hours or days. There is a RAPD and optic disc swelling, frequently with peripapillary hemorrhages. Gradually over weeks the optic disc develops pallor, and the edema resolves. Occasionally, disc swelling may be seen prior to visual loss (incipient AION). The typical visual field defect is altitudinal or arcuate, especially inferiorly.

Acutely, some patients develop “luxury perfusion” of the ischemic optic nerve head, seen as dilated capillaries on the disc edema, or adjacent to the optic nerve pallor (▶Fig. 8.20).
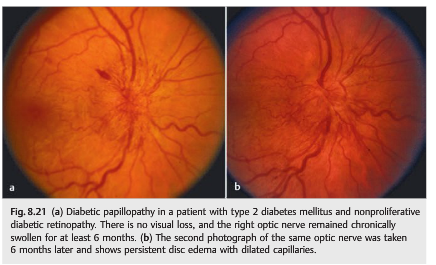
Diabetic papillopathy is believed to be an atypical form of AION that usually occurs in young patients with insulin-dependent diabetes. It is distinguished from typical nonarteritic AION by the slight degree (or even absence) of visual loss, the frequency of bilateral involvement (50%), the long duration of disc edema, and the good visual outcome (▶Fig. 8.21).
Causes
Although nonarteritic AION results from vascular occlusive disease of small vessels supplying the anterior portion of the optic nerve, its exact cause remains unclear. Anatomical factors such as a congenitally small and crowded optic nerve head with a small cup-to-disc ratio (so-called disc-at-risk) may mechanically contribute to the vascular event. As a disease of the small vessels, nonarteritic AION is not associated with ipsilateral internal carotid artery stenosis, and embolic AION is extremely rare.
Risk Factors
Proposed risk factors for nonarteritic AION include the following:
● Small, crowded disc (disc-at-risk)
● Other abnormalities localized to the disc
○ Optic nerve head drusen
○ Anomalous disc
○ Severe papilledema
● Severe hypotension
○ Operative
○ Systemic massive hemorrhage
○ Cardiac arrest
○ Renal dialysis
● Severe anemia
● Hypercoagulable disorders
● Radiation optic neuropathy
● Acute intraocular hypertension (during ocular surgery, after an intravitreal injection of steroids, or during an attack of angle-closure glaucoma)
● Vascular risk factors for atherosclerosis are commonly found in AION patients.
In rare cases, AION may occur in a patient with optic nerve head drusen or papilledema. The drusen or the papilledema makes the optic nerve head more crowded and may “choke” the optic nerve head, which becomes ischemic (▶Fig. 8.23). Medications, such as amiodarone, may induce an optic neuropathy often indistinguishable from AION.

Pearls
Nonarteritic AION is not an embolic disorder. Evaluation of the internal carotid artery is not indicated in isolated, typical AION. There is no definite increased risk of cerebrovascular disease in the population of patients with AION, but vascular risk factors are common and should be controlled.
Natural History
Up to 50% of patients retain visual acuity of 20/60 or better. Recurrences in the same eye are rare (<5%). Subsequent involvement of the fellow eye is about 15% at 5 years in patients with a disc-at-risk.
Treatment
There is no established treatment for nonarteritic AION. The clinician’s primary role is to exclude giant cell arteritis, control vascular risk factors, treat anemia, and prevent hypotension (e.g., in the setting of dialysis).
8.5.4 Nonarteritic Posterior Ischemic Optic Neuropathy
Characteristics
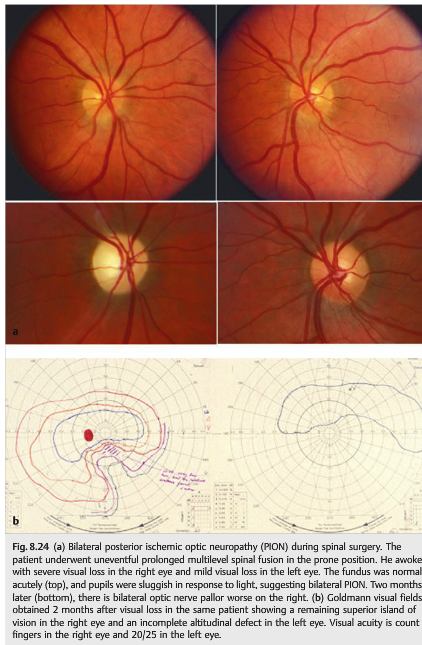
Nonarteritic PION (▶Fig. 8.24) is characterized by acute, painless monocular loss of vision that may progress over several hours or days. There is a RAPD. The optic disc is normal, initially. Gradually, over 4 to 6 weeks, the optic disc develops pallor. The typical visual field defect is altitudinal or arcuate, especially inferiorly.
Diagnosis and Causes
Nonarteritic PION is extremely rare and may occur during lengthy spinal and cardiac surgery or in patients with acute systemic hypotension. It is usually a diagnosis of exclusion made only after compression of the posterior optic nerve is ruled out by a good-quality MRI scan of the orbits with contrast, along with an extensive systemic workup looking for an underlying systemic inflammatory disorder. Non operative PION in patients older than age 50 is usually indicative of giant cell arteritis.
Risk Factors
Presumed risk factors for nonarteritic PION include the following:
● Operative
○ Spine (prone; long duration)
○ Coronary artery bypass
● Severe hypotension
○ Systemic hemorrhage
○ Cardiac arrest
○ Renal dialysis
● Severe anemia
● Hypercoagulable disorders
● Radiation optic neuropathy
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.