Question: What are 7 indications for B-scan echography?
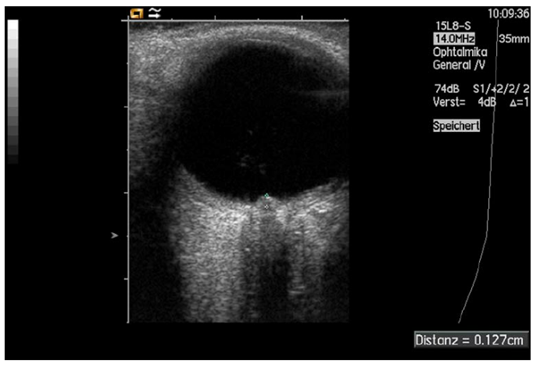
Fig. 8. Measurement of papilledema using ultrasound: disc elevation is quantified by putting the first caliper on the uppermost part of the swollen disc; the second caliper is positioned on the strongly reflecting line representing the lamina cribrosa 8
 1
1
 1
1 1
1 1
1 1
1 1
1 1
1 1
1