Questions:
1. In the photostress test, how long does the patient look at a bright light held a few centimeters from the eye?
2. In the photostress test, what is the normal recovery time to within 1 line of best corrected visual acuity?
3. What anatomic factor explains the RAPD with an optic tract lesion?
4. What are 5 clinical settings where OKN testing may be helpful?
5. Where is the lesion likely to be located in a patient with homonymous hemianopia and asymmetric OKN response?
 1
1
____________________________________________________
Questions with answers:
1. In the photostress test, how long does the patient look at a bright light held a few centimeters from the eye?
10 seconds
2. 2. In the photostress test, what is the normal recovery time to within 1 line of best corrected visual acuity?
30 seconds or less
3. What anatomic factor explains the RAPD with an optic tract lesion?
The nasal fibers of one eye (53% of all fibers) cross in the chiasm to join the uncrossed temporal fibers (47% of all fibers) of the contralateral eye. Because more fibers in the optic tract come from the contralateral eye (crossed fibers), a relative afferent pupillary defect is often observed in the eye contralateral to an optic tract lesion.
4. What are 5 clinical settings where OKN testing may be helpful?
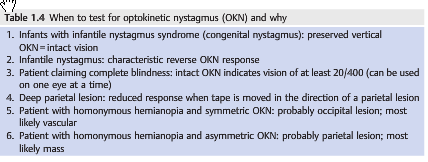
-1. Reduced visual acuity: OKN response confirms the presence of 20/400 of better VA (useful forinfants, very young children, & patients suspected of nonorganic visual loss claiming to have a visual acuity less than 20/400).
-2. The diagnosis of infantile nystagmus: a preserved vertical OKN response indicates intact vision and there is typically a reverse response to horizontal OKN.
-3. The diagnosis of internuclear ophthalmoplegia, OKN is helpful in eliciting subtle adduction weakness.
-4. The diagnosis of the dorsal midbrain syndrome: rotate the drum downward to elicit its convergence retraction nystagmus, and
-5. Localizing a homonymous hemianopia: A reduced OKN response when moving the OKN tape in the direction of a deep parietal lobe lesion is often present, in other locations it will be normal.
5. Where is the lesion likely to be located in a patient with homonymous hemianopia and asymmetric OKN response?
Probably deep in the parietal lobe (most likely mass). There is a reduced response when OKN tape is moved in the direction of the lesion.
Explanation1:
1.4 Photostress Recovery Test
Photostress recovery is used to differentiate between macular disease and optic neuropathy. The principle underlying this test is that recovery of retinal sensitivity following exposure to a bright light is based on regeneration of visual pigments that were bleached during exposure to light. A delay in this process occurs in diseases affecting the photoreceptors and is independent of the neural pathways.
Each eye is tested separately:
1. Measure the best corrected visual acuity in each eye.
2. Have the patient look directly into a bright light held a few centimeters from the eye for 10 seconds.
3. Record the time taken for the visual acuity to return to within one line of the best corrected visual acuity.Most normal patients will have a recovery time less than 30 seconds, which is symmetric between the two eyes. Macular diseases (but not optic neuropathies) often cause a prolongation in the photostress recovery time. This is particularly useful for unilateral or subtle macular diseases.
1.5 Amsler Grid
The Amsler grid is very useful in detecting macular abnormalities as a cause of visual loss.
Each eye is tested separately, and the patient is asked to fixate on a central point in a square grid of lines and to draw any area in which the lines disappear or are broken, warped, double, or curved.
Patients with maculopathy often see the straight lines as curved (metamorphopsia).
1.6 Stereo Vision
Stereo vision is tested on a specific book (Titmus test) with both eyes open and polarized glasses placed on the patient’s reading corrective lenses. This book shows animals and circles that are seen in stereo with the polarized glasses.
Stereopsis requires binocular vision. Therefore, the presence of stereopsis indicates at least some vision in each eye. This test is very helpful when nonorganic visual loss is suspected.
Stereopsis can be quantified and correlated with visual acuity (▶Table 1.2).
1.11 Ocular Motility
“The motility examination evaluates the integrity of the following:
● Extraocular muscles
● Neuromuscular junction
● Ocular motor nerves (third, fourth, and sixth)
● Ocular motor nuclei
● Internuclear pathways
● Supranuclear pathways
The ocular motility examination consists of the following:
● Observation in primary gaze
● Ductions (monocular eye movements)
● Vergence (binocular dysconjugate movements)
● Versions (binocular conjugate eye movements)
○ Saccades○ Pursuit
○ Oculocephalic responses and vestibulo-ocular reflex (VOR)
○ Optokinetic nystagmus
● Detection and measurement (with prisms) of ocular misalignment (strabismus)
● Detection of nystagmus
The various techniques used to examine the extraocular movements, how to interpret abnormal extraocular movements, and their localization value are detailed in Chapter 13.
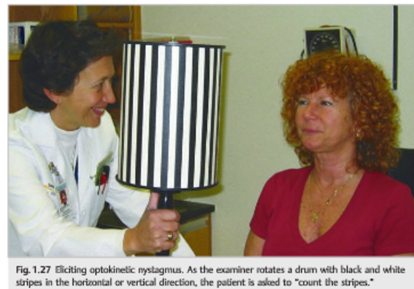
An optokinetic stimulus produces a jerk nystagmus in patients with good vision and intact ocular motor systems. It coordinates eye movements when the environment moves, such as when looking out from a moving train.
Physiologic optokinetic nystagmus (OKN) can be elicited by rotating a striped drum or moving a striped tape horizontally and vertically and asking the patient to “count the stripes as they go by” (▶Fig. 1.27).

The slow phases of the OKN are generated as the patient follows a target. The OKN fast phase is a corrective saccade to view the next target.The OKN response is involuntary and is difficult to suppress. An intact OKN response confirms that visual acuity is at least 20/400. This is very helpful in checking the vision of infants and very young children as well as patients suspected of loss claiming to have a visual acuity of hand motion, light perception, or no light perception. ▶Table 1.4 outlines when to test for OKN and why. Testing the OKN is also helpful to elicit subtle adduction weakness in internuclear ophthalmoplegia and convergence retraction nystagmus of the dorsal midbrain syndrome (rotate the drum downward).nonorganic visual loss claiming to have a visual acuity of hand motion, light perception, or no light perception. ▶Table 1.4 outlines when to test for OKN and why. Testing the OKN is also helpful to elicit subtle adduction weakness in internuclear ophthalmoplegia and convergence retraction nystagmus of the dorsal midbrain syndrome (rotate the drum downward).”1
Reference:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.