Questions:
11. What is the Tolosa-Hunt syndrome?
12. Where do these findings localize the lesion: Nystagmus, skew deviation, ocular tilt reaction, vertigo, lateropulsion, ipsilateral Horner syndrome, cerebellar syndrome, facial hypoesthesia, cranial nerves IX and X, and contralateral pain and thermal hypoesthesia (Wallenberg syndrome)?
13. Where do these findings localize the lesion: 4th nerve palsy with contralateral Horner syndrome?
14. Where do these findings localize the lesion: 3rd nerve palsy with contralateral ptosis and contralateral superior rectus weakness?
15. Where do these findings localize the lesion: 3rd nerve palsy with contralateral hemiparesis (Weber syndrome)?
16. Where do these findings localize the lesion: 3rd nerve palsy and ipsilateral cerebellar ataxia (Nothnagel syndrome)?
17. Where do these findings localize the lesion: 3rd nerve palsy and contralateral tremor (Benedikt syndrome)?
18. Where do these findings localize the lesion: 3rd nerve palsy and contralateral ataxia with tremor (Claude syndrome)?
19. Where do these findings localize the lesion: 3rd nerve palsy with vertical gaze palsy, lid retraction, skew deviation, and convergence nystagmus?
20. Where do these findings localize the lesion: 3rd nerve palsy with depressed mental status?
Archives for 2018
Neuro-ophthalmology Questions of the Week: NOI13 Diplopia10.2 – Other Eye Movement Abnormalities
Pearls and oy-sters of localization in ophthalmoparesis
Pearls and oy-sters of localization in ophthalmoparesis
Teresa Buracchio, Janet C. Rucker
Neurology. December 11, 2007; 69 (24) RESIDENT AND FELLOW SECTION
Abstract
Ocular misalignment and ophthalmoparesis result in the symptom of binocular diplopia. In the evaluation of diplopia, localization of the ocular motility disorder is the main objective. This requires a systematic approach and knowledge of the ocular motor pathways and actions of the extraocular muscles. This article reviews the components of the ocular motor pathway and presents helpful tools for localization and common sources of error in the assessment of ophthalmoparesis.
Neuro-ophthalmology Questions of the Week: NOI13 Diplopia10.1 – Other Eye Movement Abnormalities
Questions:
1. What are the findings of the Locked-in Syndrome?
2. Where is the lesion in the Locked-in Syndrome?
3. What is Ocular Neuromyotonia?
4. What are the symptoms of Ocular Neuromyotonia?
5. What is the usual cause of Ocular Neuromyotonia?
6. Where do these findings localize the lesion: Horizontal gaze palsy with ipsilateral facial palsy?
7. Where do these findings localize the lesion: 6th nerve palsy with contralateral hemiparesis (Raymond syndrome)?
8. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral seventh nerve palsy and contralateral hemiparesis (Millard-Gubler syndrome)?
9. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral seventh nerve palsy, deafness, hypoesthesia, Horner syndrome, contralateral pain and thermal hypoesthesia, ataxia (Foville syndrome)?
10. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral Horner Syndrome?
Teaching Video NeuroImages: Alternating skew deviation with abducting hypertropia following superior colliculus infarction
Teaching Video NeuroImages: Alternating skew deviation with abducting hypertropia following superior colliculus infarction
Damien Biotti, Marianne Barbieux and David Brassat
Neurology. March 01, 2016; 86 (9) RESIDENT AND FELLOW SECTION
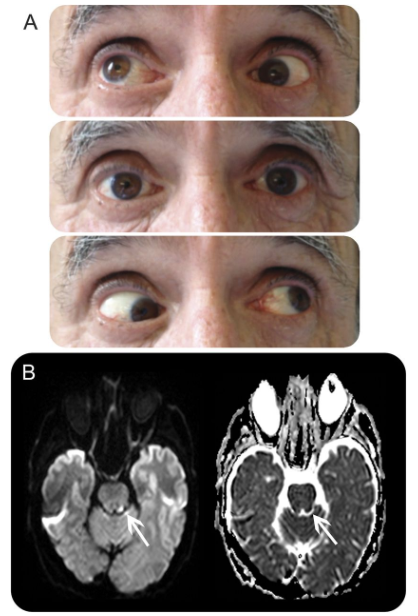
A 63-year-old patient was admitted with acute ataxia and binocular oblique diplopia. Neuro-ophthalmologic examination revealed abducting hypertropia on lateral gaze, better seen during upgaze, mimicking bilateral inferior oblique palsy (Figure A, video). There was no ocular cyclotorsion. Brain MRI revealed focal ischemic lesions in the right cerebellar hemisphere and left superior colliculus (Figure B). The diagnosis of alternating abducting hypertrophic skew deviation was made. This rare type of skew deviation is related to central otolithic dysfunction. Similar cases have been described with cerebellar, pretectal, or cervico-medullary junction lesions.1,2 Orthoptic management can help and patients can slowly improve over months.
Figure Ocular motor examination and MR images
(A) Ocular motor examination (right gaze, straight gaze, left gaze).
(B) Diffusion-weighted imaging (left) and apparent diffusion coefficient images (right) reveal a focal and acute ischemic stroke.
AUTHOR CONTRIBUTIONS D. Biotti: principal author, corresponding author. M. Barbieux: contributor, neurologic management. D. Brassat: contributor.
STUDY FUNDING No targeted funding reported.
DISCLOSURE The authors report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
Footnotes
● Go to Neurology.org for full disclosures. Funding information and disclosures deemed relevant by the authors, if any, are provided at the end of the article.
● Supplemental data at Neurology.org
● Download teaching slides: Neurology.org
REFERENCES
1. Versino M, Hurko O, Zee D. Disorders of binocular control of eye movements in patients with cerebellar dysfunction. Brain 1996;119:1933–1950.
2. Hamed LM, Maria BL, Quisling RG, Mickle JP. Alternating skew on lateral gaze: neuroanatomic pathway and relationship to superior oblique overaction. Ophthalmology 1993;100:281–286.
Neuro-ophthalmology questions of the week: NOI13 Diplopia 9.4 – Internuclear & Supranuclear Lesions
Questions:
38. Where are eye movements initiated?
39. Which of the following can cause a patient to be unable look to the left?
A. Right FEF, B. Left FEF, C. Right PPRF, D. Left PPRF
40. Where are smooth pursuit eye movements generated?
41. What is the function of inputs to the visual system from the vestibular nuclear complexes?
42. What is the cause of skew deviation?
Teaching Video NeuroImages: Minimal anomalies of dorsal midbrain syndrome (Parinaud syndrome)
Teaching Video NeuroImages: Minimal anomalies of dorsal midbrain syndrome (Parinaud syndrome)
Pilar Rojas, Philippe Maeder and François-Xavier Borruat.
Neurology. January 03, 2017; 88 (1) RESIDENT AND FELLOW SECTION
Parinaud syndrome results from posterior commissure dysfunction, and is associated with 4 major signs: limitation of upgaze, pupillary light-near dissociation, convergence abnormalities, and Collier sign.1,2
A 46-year-old man complained of vertical diplopia due to a subtle left skew deviation. Upgaze pursuit was normal, but upward saccades were slowed, without convergence abnormalities or Collier sign (video). Pupillary light-near dissociation was present (video). MRI revealed a tectal mesencephalic lesion (figure).
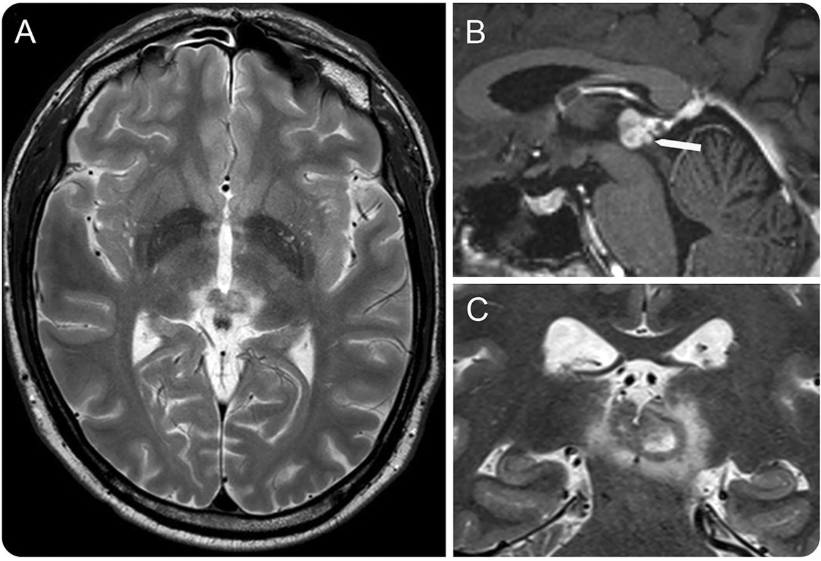
Figure Brain MRI
T2 axial and coronal cuts (A, C) and T1 sagittal cut with gadolinium (B) revealed a tumor originating from the walls of the third ventricle posteriorly, with an invasion of the posterior commissure (white arrow). The lesion was later biopsied and pathology revealed a pilocytic astrocytoma.
Video Ocular motility and pupils examination.
Horizontal pursuit and saccades, and both upward and downward vertical pursuit were normal in both eyes, namely without any limitation of upgaze. The speed of downward vertical saccades was normal, whereas upward saccades from primary gaze were slowed. The pupils were of intermediate and equal size, and pupillary light-near dissociation was present in both eyes.
Slowed upward saccades and pupillary light-near dissociation represent an early stage of posterior commissure dysfunction, before frank upgaze palsy, Collier sign, or convergence abnormalities.
AUTHOR CONTRIBUTIONS
Pilar Rojas is an author and contributed to drafting and revising the manuscript. Philippe Maeder is an author, contributed to data acquisition, and revised the manuscript. François-Xavier Borruat is an author, contributed to data acquisition, and revised the manuscript.
STUDY FUNDING No targeted funding reported.
DISCLOSURE The authors report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
Footnotes
Supplemental data at Neurology.org
Download teaching slides: Neurology.org
REFERENCES
1. Leigh RJ, Zee DS. The Neurology of Eye Movements, 3rd ed. part II, ch 10. Oxford: Oxford University Press; 1999:517–519.
2. Miller NR, Newman NJ. Clinical Neuro-Ophthalmology, 5th ed. vol 1, ch 29. Baltimore: Williams & Wilkins; 1998:1304–1311.
Neuro-ophthalmology questions of the week: NOI13 Diplopia 9.3 – Internuclear & Supranuclear Lesions
Questions:
25. Where are the critical supranuclear structures mediating vertical gaze located?
26. What are the 4 most important pretectal areas related to vertical eye movement?
27. Where are the burst neurons responsible for vertical saccades located?
28. What serves as the neural integrator for vertical gaze and torsion?
29. For downgaze, where do the axons from the interstitial nucleus of Cajal (INC) project?
30. What are the 4 findings of the Dorsal Midbrain Syndrome?
31. What are 2 other names for the Dorsal Midbrain Syndrome?
32. What is a common cause of the Dorsal Midbrain Syndrome?
33. What are the characteristics of Skew Deviation?
34. What test can help differentiate a 4th nerve palsy from skew deviation?
35. What is the ocular tilt reaction?
36. What transmission pathway is disrupted in skew deviation and the ocular tilt reaction?
37. What infectious condition can cause a vertical gaze palsy?
Teaching NeuroImage: Convergence spasm associated with midbrain compression by cerebral aneurysm
Teaching NeuroImage: Convergence spasm associated with midbrain compression by cerebral aneurysm
Konrad P. Weber, Matthew J. Thurtell, and G. Michael Halmagyi
Neurology. April 08, 2008; 70 (15) RESIDENT AND FELLOW SECTION
ARTICLE
A 72-year-old woman presented with intermittent diplopia. She had a history of vascular disease, but no history of stroke or psychiatric disturbance. On examination, she developed convergence spasm with associated miosis following fixation on near targets and during horizontal smooth pursuit (video, figure 1). The spasms were terminated with a blink. She had no ptosis, her eye movements were normal in range, and her pupils were equal in size with normal reactions to light. Neurologic examination was otherwise unremarkable. Five years prior to her current presentation, a left-sided terminal carotid artery aneurysm had been incidentally detected. The aneurysm gradually expanded to a diameter of 2.4 cm and compressed the midbrain (figure 2). The intermittent diplopia had developed in the months following endovascular coiling of the aneurysm.
Figure 1 (A–D) Convergence spasm precipitated by fixation on a near target and released after a blink (video, A).
(A) During fixation on a distant target, the patient has mid-range pupils.
(B) During fixation on a near target, the patient converges and has miotic pupils.
(C) After the near target is removed, convergence is maintained. The pupils remain miotic, which helps to differentiate from bilateral sixth nerve palsies.
(D) After a blink, the patient is able to re-fixate on the distant target and the pupils return to mid-range diameter.
(E) Binocular search coil recording during sinusoidal horizontal smooth pursuit, in which there is a period of convergence spasm that is released by a blink (video, B).
(F) The vergence angle progressively increases up to 50° during the period of convergence spasm (gray triangle).
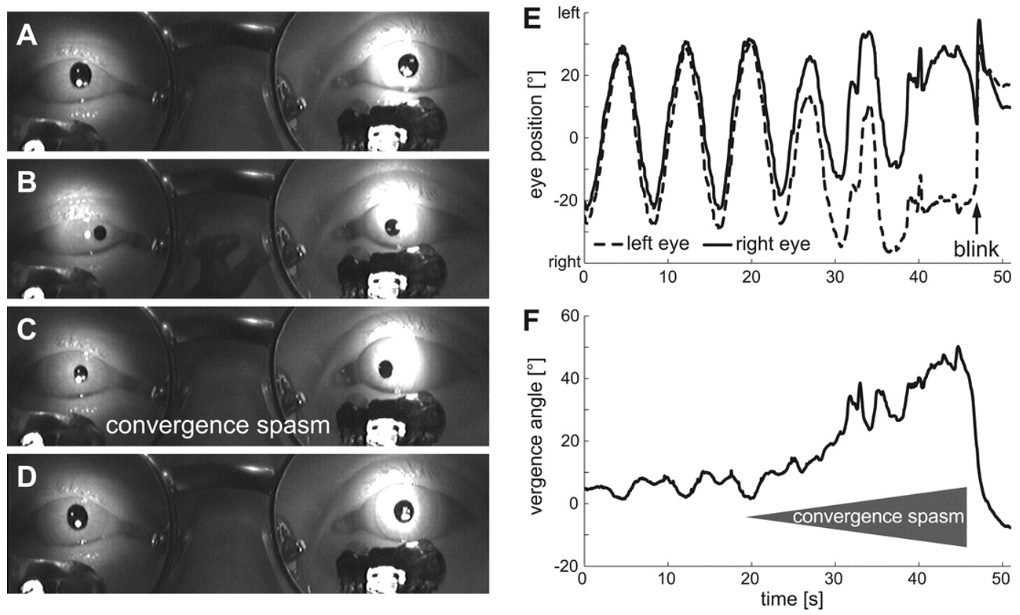
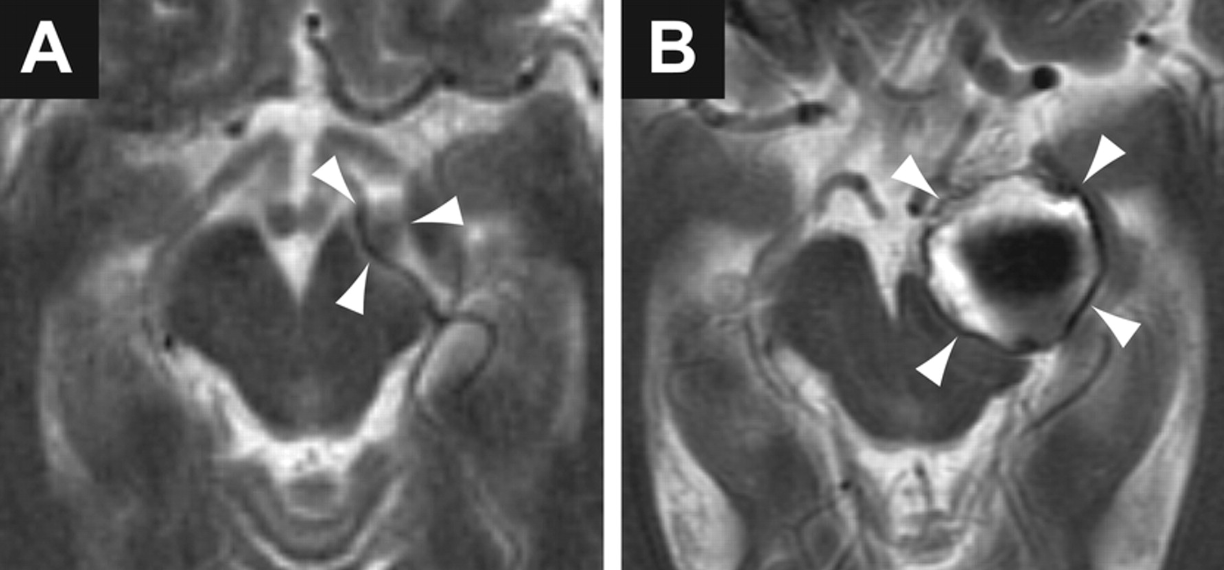
Figure 2 T2-weighted axial MRI demonstrating progressive compression of the midbrain by an expanding aneurysm (arrowheads) arising from the terminal left carotid artery
(A) MRI 5 years prior to onset of symptoms.
(B) MRI at the time of presentation with convergence spasm (after endovascular coiling of the aneurysm).
Convergence spasm is characterized by the inappropriate appearance of the near triad, which consists of convergence, miosis, and accommodation.1 Most patients are young and the cause is psychiatric; a focal lesion is rarely found.1 Since the neural substrate for the near triad is located in the midbrain, convergence spasm could occur with a midbrain lesion. In our patient, isolated convergence spasm may have been a manifestation of midbrain compression. Thus, in patients presenting with convergence spasm, the presence of other focal neurologic signs or the absence of psychiatric history, especially in the elderly, should prompt neuroimaging. Furthermore, it is important not to mistake convergence spasm for bilateral sixth nerve palsies; miosis on attempted lateral gaze is diagnostic of convergence spasm.2
ACKNOWLEDGMENT The authors thank Dr. Geoffrey D. Parker for help with the interpretation of the MRI.
Footnotes
Supplemental data at www.neurology.org
Supported by Garnett Passe and Rodney Williams Memorial Foundation.
Disclosure: The authors report no conflicts of interest.
Series editor: Mitchell S.V. Elkind MD, MS, Section Editor
REFERENCES
1. Goldstein JH, Schneekloth BB. Spasm of the near reflex: a spectrum of anomalies. Surv Ophthalmol. 1996;40:269–278
2. Griffin JF, Wray SH, Anderson DP. Misdiagnosis of spasm of the near reflex. Neurology. 1976;26:1018–1020
Neuro-ophthalmology questions of the week: NOI13 Diplopia 9.2 – Internuclear & Supranuclear Lesions
Questions:
15. What is ocular apraxia?
16. What is convergence spasm?
17. What is the cause of convergence spasm?
18. What test will usually differentiate convergence spasm from a bilateral 6th nerve palsy?
19. What is convergence insufficiency?
20. How is convergence insufficiency treated?
21. What are causes of convergence insufficiency?
22. What is divergence insufficiency?
23. What causes divergence insufficiency?
24. What lesion location is likely in the presence of horizontal conjugate deviation of the eyes to one side?
Teaching Video NeuroImages: Pulsatile proptosis and wall-eyed bilateral internuclear ophthalmoplegia
Teaching Video NeuroImages: Pulsatile proptosis and wall-eyed bilateral internuclear ophthalmoplegia
Eleni Papageorgiou, Evangelia E. Tsironi, Sofia Androudi and Petros Koltsidopoulos
Neurology. April 24, 2018; 90 (17) RESIDENT & FELLOW SECTION
ARTICLE
A 65-year-old man with a history of hypertension presented with double vision. Examination revealed wall-eyed bilateral internuclear ophthalmoplegia (WEBINO) (figure 1) and nonsymptomatic, pulse-synchronous, pulsatile proptosis of the left eye (video, links.lww.com/WNL/A389). According to the patient, there was a history of blunt head trauma in childhood and the pulsatile eye was present since then. CT revealed a meningocele into the left orbit due to a bony defect in the orbital roof (figure 2A). CT angiography ruled out a carotid-cavernous fistula. MRI showed an acute infarction at the midline of the midbrain tegmentum, which involved the medial longitudinal fasciculus bilaterally and caused the WEBINO (figure 2B).1 The pulsatile proptosis was attributed to the childhood head injury and due to the orbital roof fracture and associated meningocele pulsation of the brain vessels passed onto the CSF.2
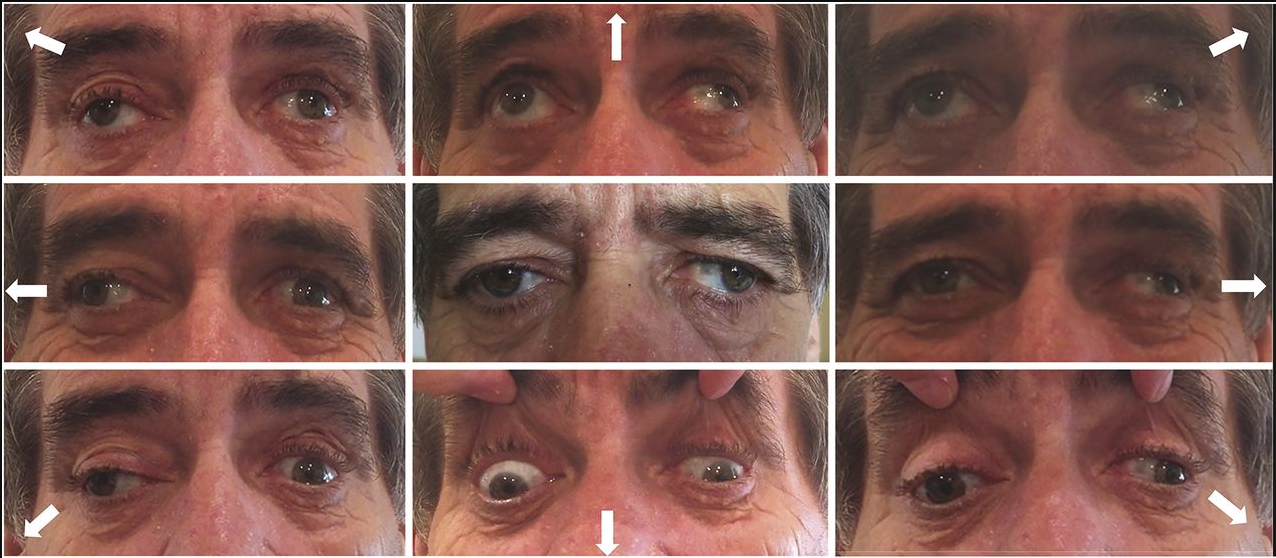
Figure 1 Extraocular movements in 9 cardinal gaze positions
Extraocular eye movements demonstrate exotropia of both eyes in primary positions and bilateral internuclear ophthalmoplegia with impaired adduction on attempted lateral gaze. Upgaze is also mildly affected.
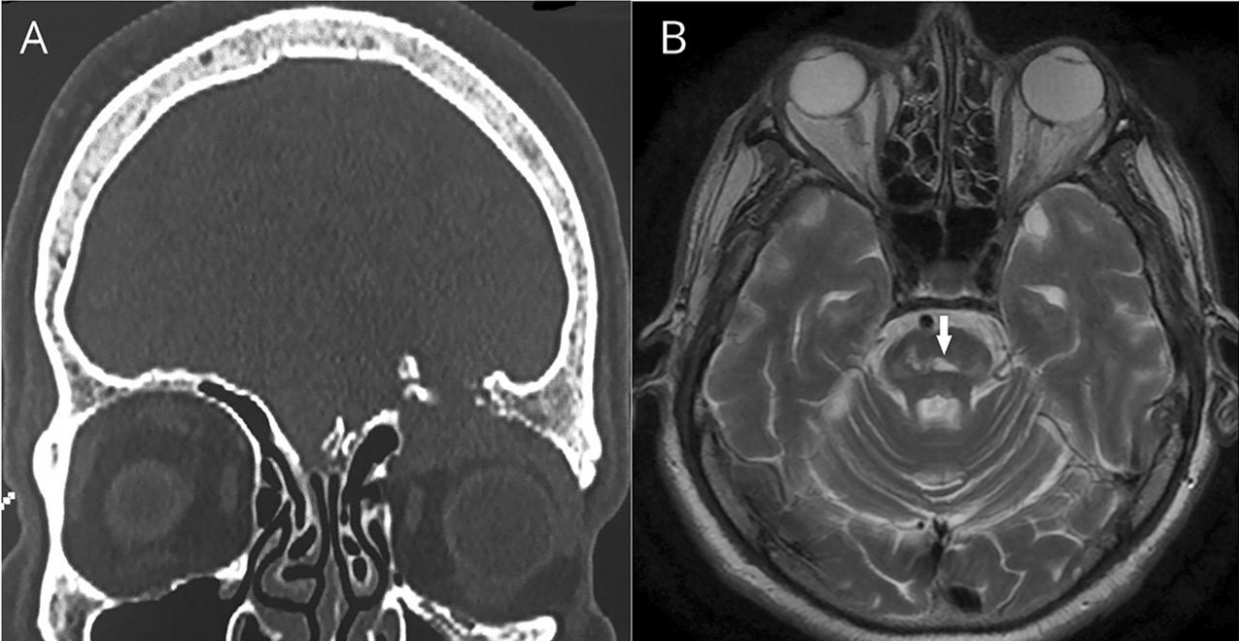
Figure 2 Coronal brain CT and axial brain MRI
(A) Coronal brain CT shows fracture of the left orbital roof with an associated meningocele.
(B) T2-weighted axial brain MRI demonstrates an acute infarction at the midline of the midbrain tegmentum, which involves the medial longitudinal fasciculus bilaterally.
Author contributions E.P.: study concept and design, acquisition of data, analysis and interpretation, writing of the manuscript. E.E.T. and S.A.: study supervision, critical revision of the manuscript for important intellectual content. P.K.: acquisition of data, analysis and interpretation.
Study funding No targeted funding reported.
Disclosure The authors report no disclosures relevant to the manuscript.
References:
1. Kim JS, Jeong SH, Oh YM, Yang YS, Kim SY. Teaching NeuroImage: wall-eyed bilateral internuclear ophthalmoplegia (WEBINO) from midbrain infarction. Neurology 2008;70:e35.
2. Chousterman B, Gualino V, Dohan A, Payen D. A mysterious post-traumatic pulsatile exophthalmos. Intens Care Med 2014;40:102–103.