Questions:
25. Where are the critical supranuclear structures mediating vertical gaze located?
26. What are the 4 most important pretectal areas related to vertical eye movement?
27. Where are the burst neurons responsible for vertical saccades located?
28. What serves as the neural integrator for vertical gaze and torsion?
29. For downgaze, where do the axons from the interstitial nucleus of Cajal (INC) project?
30. What are the 4 findings of the Dorsal Midbrain Syndrome?
31. What are 2 other names for the Dorsal Midbrain Syndrome?
32. What is a common cause of the Dorsal Midbrain Syndrome?
33. What are the characteristics of Skew Deviation?
34. What test can help differentiate a 4th nerve palsy from skew deviation?
35. What is the ocular tilt reaction?
36. What transmission pathway is disrupted in skew deviation and the ocular tilt reaction?
37. What infectious condition can cause a vertical gaze palsy?
____________________________________________________
Questions with answers:
25. Where are the critical supranuclear structures mediating vertical gaze located?
The critical supranuclear structures mediating vertical gaze are located in the rostral midbrain at the level of the pretectum (just rostral to the superior and inferior colliculi).
26. What are the 4 most important pretectal areas related to vertical eye movement?
1. the rostral interstitial nucleus of the MLF (riMLF)
2. the interstitial nucleus of Cajal (INC)
3. the nucleus of the posterior commissure
4. the posterior commissure
27. Where are the burst neurons responsible for vertical saccades located?
The burst neurons responsible for vertical saccades are located in the paramedian rostral interstitial nucleus of the MLF (riMLF).
28. What serves as the neural integrator for vertical gaze and torsion?
The interstitial nucleus of Cajal (INC) serves as the neural integrator for vertical gaze and torsion.
29. For downgaze, where do the axons from the interstitial nucleus of Cajal (INC) project?
For downgaze, the axons from the interstitial nucleus of Cajal (INC) project to the ipsilateral inferior rectus subnucleus and 4th nerve nucleus.
29. What are the 4 findings of the Dorsal Midbrain Syndrome?
1. Supranuclear vertical up gaze paresis
2. Convergence retraction nystagmus with attempted up gaze
3. Lid retraction (Collier’s sign)
4. Pupillary light-near dissociation
31. What are 2 other names for the Dorsal Midbrain Syndrome?
Parinaud syndrome and the pretectal syndrome
32. What is a common cause of the Dorsal Midbrain Syndrome?
Obstructive hydrocephalus is a common cause of the dorsal midbrain syndrome.
33. What are the characteristics of Skew Deviation?
Skew deviation is an acquired vertical misalignment of the eyes resulting from asymmetric disruption of supranuclear input from the otolithic organs.
It commonly results from acute brainstem/cerebellar dysfunction.
Patients complain of vertical diplopia, sometimes with a torsional component (an exception to the general rule that supranuclear lesions do not produce diplopia).
There are usually other neurologic symptoms (e.g. ataxia).
The hypertropia of a skew deviation may be comitant or incomitant.
When a skew deviation is comitant, it may be difficult to distinguish from a third nerve palsy or a fourth nerve palsy.
Ocular torsion and head tilt may accompany a skew deviation (ocular tilt reaction).
34. What test can help differentiate a 4th nerve palsy from skew deviation?
The upright-supine test helps differentiate a skew deviation from trochlear nerve palsy: a vertical deviation that decreases by ≥50% from the upright to supine position suggests a skew deviation.
35. What is the ocular tilt reaction?
A combination of:
1. Skew deviation
2. Ocular torsion (both eyes are tilted/tilted toward the hypotropic eye)
3. Head tilt (toward the hypotrophic eye).
36. What transmission pathway is disrupted in skew deviation and the ocular tilt reaction?
The otolith-ocular pathway of the vestibular nerves, the brainstem, or the cerebellum.
37. What infectious condition can cause a vertical gaze palsy?
Whipple disease can present as a vertical gaze palsy. This rare disorder is often discussed in neuro-ophthalmology because it is frequently associated with eye movement abnormalities.
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
Control of Vertical Eye Movements (▶Fig. 13.122 and ▶Fig. 13.123a&b)
Control of vertical eye movements include the following:
● Critical supranuclear structures mediating vertical gaze are located in the rostral midbrain at the level of the pretectum (just rostral to the superior and inferior colliculi).
● The four most important pretectal areas are the rostral interstitial nucleus of the MLF (riMLF), the interstitial nucleus of Cajal (INC), the nucleus of the posterior commissure, and the posterior commissure.
● The paramedian riMLF contains burst neurons responsible for vertical saccades.
● The riMLF controls upward saccades via the elevator muscles (projections to the superior rectus and inferior oblique subnuclei) and downward saccades via the depressor muscles (projections to the inferior rectus subnucleus and to the fourth nerve nucleus).
● The INC serves as the neural integrator for vertical gaze and torsion (coordinates signals from the saccadic burst neurons in the riMLF, vestibular projections coming from the vestibular nuclei via the MLF, and descending pursuit fibers).
● Some fibers cross from one side to another at the level of the pretectum via the posterior commissure.
There is still some uncertainty about projections involved in vertical eye movements, and only clinically relevant pathways are included in these simplified anatomical diagrams.
The following are shown for upward eye movement (▶Fig. 13.123a):
Fig.13.123 (a) Major pathways subserving upward eye movements (coronal view).
INC, interstitial nucleus of Cajal; riMLF, rostral interstitial nucleus of the medial longitudinal fasciculus; III, third nerve nucleus; IV, IVth nerve nucleus; PC, posterior chamber.


● Neurons from the riMLF (and nucleus of the posterior commissure), which contains burst neurons for vertical saccades, project both ipsilaterally and contralaterally to the oculomotor nuclear complexes, innervating the superior rectus and the inferior oblique subnuclei bilaterally.
● Axons from the INC, the neural integrator for vertical gaze, cross within the posterior commissure before reaching the oculomotor nuclear complexes and the superior rectus and inferior oblique subnuclei.
The following are shown for downward eye movement (▶Fig. 13.123b):
Fig.13.123 (b) Major pathways subserving downward eye movements (coronal view).
INC, interstitial nucleus of Cajal; riMLF, rostral interstitial nucleus of the medial longitudinal fasciculus; III, third nerve nucleus; IV, IVth nerve nucleus; PC, posterior chamber.
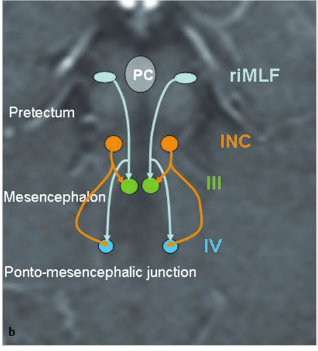
● For down gaze, each riMLF supplies the ipsilateral inferior rectus subnucleus and the ipsilateral fourth nerve nucleus (which innervates the contralateral superior oblique muscle).
● Axons from the INC innervate the ipsilateral inferior rectus subnucleus and fourth nerve nucleus.
Vertical Eye Movement Abnormalities
Up Gaze Paresis
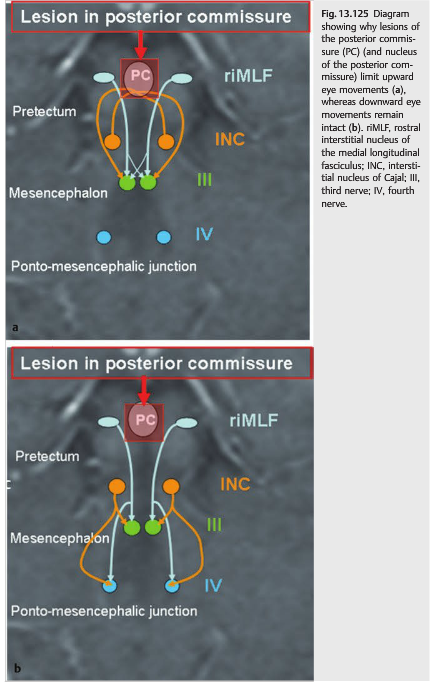
Dorsal Midbrain Syndrome(▶Fig. 13.124 and ▶Fig. 13.125) (Parinaud syndrome or pretectal syndrome) classically includes the following:
● Supranuclear vertical up gaze paresis
● Convergence retraction nystagmus with attempted up gaze
● Lid retraction (Collier sign)
● Pupillary light-near dissociation
It may be associated with any of the following:
● Pseudoabducens palsy (thalamic esotropia)
● Convergence insufficiency
● Accommodative insufficiency
● Skew deviation
● Third nerve palsy
● Internuclear ophthalmoplegia
● See-saw nystagmus
Lesions of the posterior commissure (and of the nucleus of the posterior commissure)limit upward eye movements. Convergence–retraction nystagmus with attempted up gaze results from asynchronous convergent saccades.
Lesions may also damage the pretectal (light) fibers entering the Edinger–Westphal nucleus, sparing fibers for the near response (accommodation) that enter the Edinger–Westphal nucleus more ventrally. This results in light-near dissociation of the pupils (▶Fig. 13.126).
Pearls
Obstructive hydrocephalus is a common cause of dorsal midbrain syndrome, and patients with vertical gaze deficits should have urgent neuroimaging (▶Fig. 13.127).
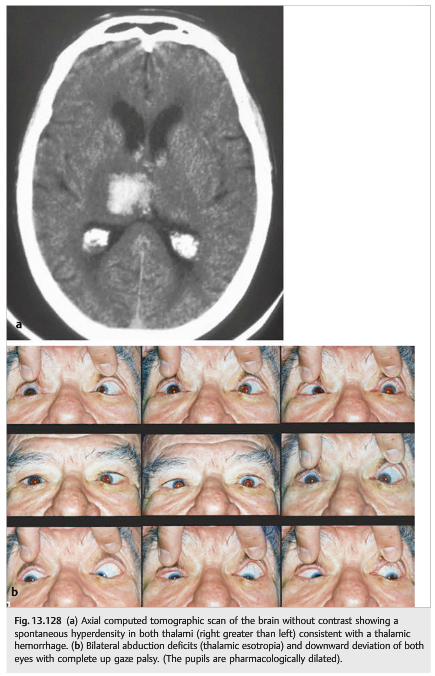
Thalamic hemorrhages classically present with sudden headache and contralateral hemisensory loss. Hemiparesis (internal capsule) and homonymous hemianopia (optic tract) may occur. Large hemorrhages can result in vertical and horizontal ocular deviations (▶Fig. 13.128).
Down Gaze Paresis
Isolated down gaze paresis due to a midbrain lesion is much less common than isolated up gaze paresis or combined up- and down gaze paresis (▶Fig. 13.125 and ▶Fig. 13.129).
● A unilateral lesion of one riMLF or its descending fibers will affect downward saccades more than upward saccades (due to the duplication of riMLF input into the oculomotor subnuclei for up gaze, but not down gaze).
● A unilateral lesion of the riMLF may cause defective torsion of the ipsilateral eye, thereby producing torsional nystagmus beating contralateral to the side of the lesion.
● Bilateral lesions of the riMLF or its descending fibers will result in a more severe defect of vertical gaze than that due to unilateral lesions. Downward saccades are typically affected more than upward saccades, but a complete vertical gaze palsy also occurs.
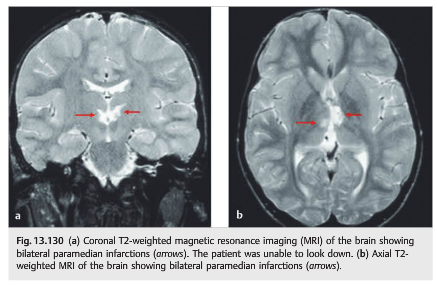
● Bilateral lesions are common, with small infarctions involving the paramedian arteries (arteries of Percheron) at the top of the basilar artery (one medial artery often vascularizes both riMLF) (▶Fig. 13.129 and ▶Fig. 13.130).
Causes of Vertical Gaze Palsy
● Lesions of the upper midbrain, pretectum, posterior commissure
○ Infarction (paramedian, thalamic, top of the basilar syndrome)
○ Hemorrhage (upper midbrain, thalamic) (hypertensive, vascular malformations)
○ Obstructive hydrocephalus
○ Pineal region tumors
– Germinoma, pineoblastoma, pineal cysts, tectal glioma
○ Basal ganglia abscess
○ Multiple sclerosis
● Progressive supranuclear palsy
● Huntington disease
● Whipple disease
● Wernicke encephalopathy
● Niemann-Pick disease
● Gaucher disease
● Tay-Sachs disease
● Wilson disease
● Paraneoplastic syndromes
Up gaze is often limited to some degree in otherwise healthy elderly patients and maybe a normal finding.
Skew Deviation and the Ocular Tilt Reaction
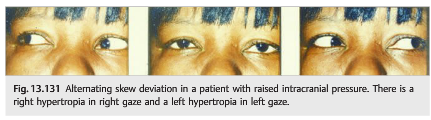
Skew deviation (▶Fig. 13.131) consists of the following:
● Vertical misalignment of the eyes commonly results from acute brainstem dysfunction.
● Patients complain of vertical diplopia, sometimes with a torsional component.
● There are usually other neurologic symptoms.
● The hypertropia of a skew deviation may be comitant (deviation is the same in all positions of gaze) or noncomitant (deviation varies with gaze position). When a skew deviation is noncomitant, it may be difficult to distinguish from a third nerve palsy or a fourth nerve palsy.
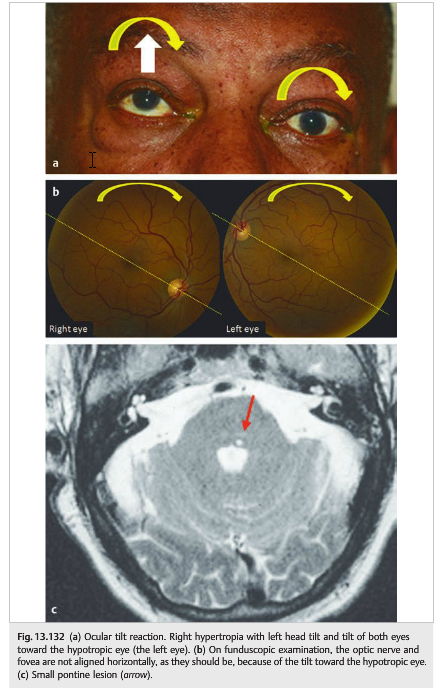
Ocular tilt reaction (OTR) (▶Fig. 13.132) is a combination of the following:
● Skew deviation
● Ocular torsion (both eyes are tilted toward the hypotropic eye) (It is easy to see the ocular torsion on funduscopic examination: the imaginary line drawn between the optic nerve and the fovea appears tilted.)
● Head tilt (toward the hypotropic eye)
● Common with lesions of the pontomedullary junction or the paramedian thalamic–mesencephalic region
● Results from dysfunction of the utricular pathways that begin in the labyrinths and terminate in the rostral brainstem at the INC
● The OTR will be
○ ipsiversive with peripheral and pontomedullary lesions
○ contraversive with pontomesencephalic lesions
Skew deviation and the ocular tilt reaction occur when there is disruption of the otolith-ocular pathway in the vestibular nerves, the brainstem, or the cerebellum.
Classic causes of skew deviation and ocular tilt reaction include the following:
● Acute peripheral vestibulopathy
○ Lesion of the vestibular organ or its nerve
○ Tullio phenomenon: sound-induced vestibular symptoms caused by a perilymph
○ Fistula or abnormalities of the ossicular chain in the ear
● Lesion in the vestibular nuclei (e.g., part of the lateral medullary syndrome)
● Lesion in the cerebellum
● Lesion in the MLF
● Lesion in the midbrain and INC
● Raised intracranial pressure




Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.