Teaching NeuroImage: Convergence spasm associated with midbrain compression by cerebral aneurysm
Konrad P. Weber, Matthew J. Thurtell, and G. Michael Halmagyi
Neurology. April 08, 2008; 70 (15) RESIDENT AND FELLOW SECTION
ARTICLE
A 72-year-old woman presented with intermittent diplopia. She had a history of vascular disease, but no history of stroke or psychiatric disturbance. On examination, she developed convergence spasm with associated miosis following fixation on near targets and during horizontal smooth pursuit (video, figure 1). The spasms were terminated with a blink. She had no ptosis, her eye movements were normal in range, and her pupils were equal in size with normal reactions to light. Neurologic examination was otherwise unremarkable. Five years prior to her current presentation, a left-sided terminal carotid artery aneurysm had been incidentally detected. The aneurysm gradually expanded to a diameter of 2.4 cm and compressed the midbrain (figure 2). The intermittent diplopia had developed in the months following endovascular coiling of the aneurysm.
Figure 1 (A–D) Convergence spasm precipitated by fixation on a near target and released after a blink (video, A).
(A) During fixation on a distant target, the patient has mid-range pupils.
(B) During fixation on a near target, the patient converges and has miotic pupils.
(C) After the near target is removed, convergence is maintained. The pupils remain miotic, which helps to differentiate from bilateral sixth nerve palsies.
(D) After a blink, the patient is able to re-fixate on the distant target and the pupils return to mid-range diameter.
(E) Binocular search coil recording during sinusoidal horizontal smooth pursuit, in which there is a period of convergence spasm that is released by a blink (video, B).
(F) The vergence angle progressively increases up to 50° during the period of convergence spasm (gray triangle).
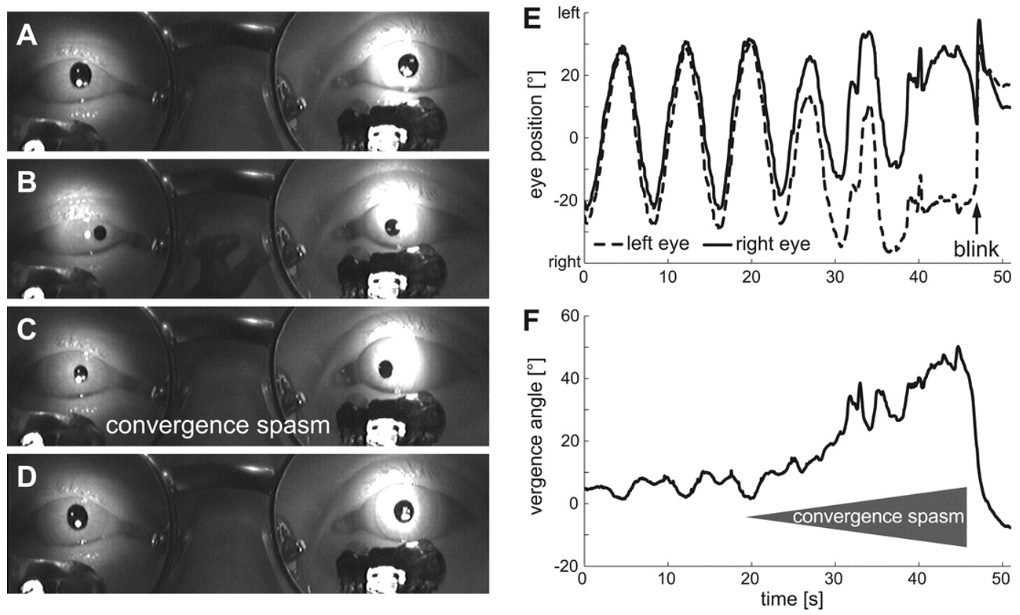
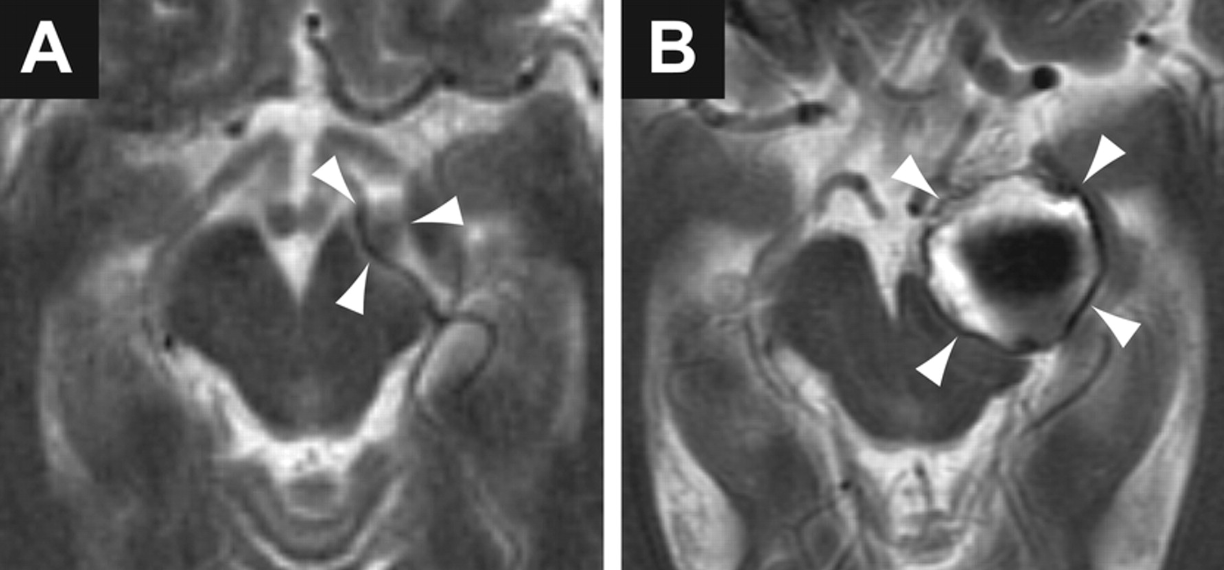
Figure 2 T2-weighted axial MRI demonstrating progressive compression of the midbrain by an expanding aneurysm (arrowheads) arising from the terminal left carotid artery
(A) MRI 5 years prior to onset of symptoms.
(B) MRI at the time of presentation with convergence spasm (after endovascular coiling of the aneurysm).
Convergence spasm is characterized by the inappropriate appearance of the near triad, which consists of convergence, miosis, and accommodation.1 Most patients are young and the cause is psychiatric; a focal lesion is rarely found.1 Since the neural substrate for the near triad is located in the midbrain, convergence spasm could occur with a midbrain lesion. In our patient, isolated convergence spasm may have been a manifestation of midbrain compression. Thus, in patients presenting with convergence spasm, the presence of other focal neurologic signs or the absence of psychiatric history, especially in the elderly, should prompt neuroimaging. Furthermore, it is important not to mistake convergence spasm for bilateral sixth nerve palsies; miosis on attempted lateral gaze is diagnostic of convergence spasm.2
ACKNOWLEDGMENT The authors thank Dr. Geoffrey D. Parker for help with the interpretation of the MRI.
Footnotes
Supplemental data at www.neurology.org
Supported by Garnett Passe and Rodney Williams Memorial Foundation.
Disclosure: The authors report no conflicts of interest.
Series editor: Mitchell S.V. Elkind MD, MS, Section Editor
REFERENCES
1. Goldstein JH, Schneekloth BB. Spasm of the near reflex: a spectrum of anomalies. Surv Ophthalmol. 1996;40:269–278
2. Griffin JF, Wray SH, Anderson DP. Misdiagnosis of spasm of the near reflex. Neurology. 1976;26:1018–1020