Questions:
1. What drops should be used to dilate the pupils for examination?
2. How long does dilation with usually last?
3. Why is it always better to dilate both eyes rather than one eye?
4. Is glaucoma a contraindication for pupillary dilation?
5. What are 5 causes of an abnormal red reflex?
6. What are 14 examples of systemic disorders in which examination of the fundus may be abnormal even without visual symptoms?
Neuro-ophthalmology Illustrated Chapter 2 Fundus Examination
December 12, 2018 By
Recommended Reading – Teaching Video NeuroImages: Oculopalatal myoclonus
December 5, 2018 By
Recommended Reading – Teaching Video NeuroImages: Oculopalatal myoclonus
Teaching Video NeuroImages: Oculopalatal myoclonus
A possible consequence of brainstem injury
Neurology. November 27, 2018; 91 (22) RESIDENT & FELLOW SECTION
A 61-year-old man with previous left cerebellar infarct complained of double vision and dizziness several months postinfarct. Infarct is shown in the figure. Examination showed rotatory nystagmus in all directions of gaze, worse on left gaze (video 1). Oral examination showed palatal tremor (video 2). Oculopalatal tremor (OPT) is thought to result from interruption of connections between the red nucleus (midbrain), dentate nucleus (cerebellum), and inferior olive (medulla).1,2 The most common cause is brainstem infarction or hemorrhage,1 but it has also been observed with multiple sclerosis and other inflammatory entities. OPT usually becomes apparent several months after the injury. Treatment may include gabapentin, memantine, benzodiazepines, and valproic acid.
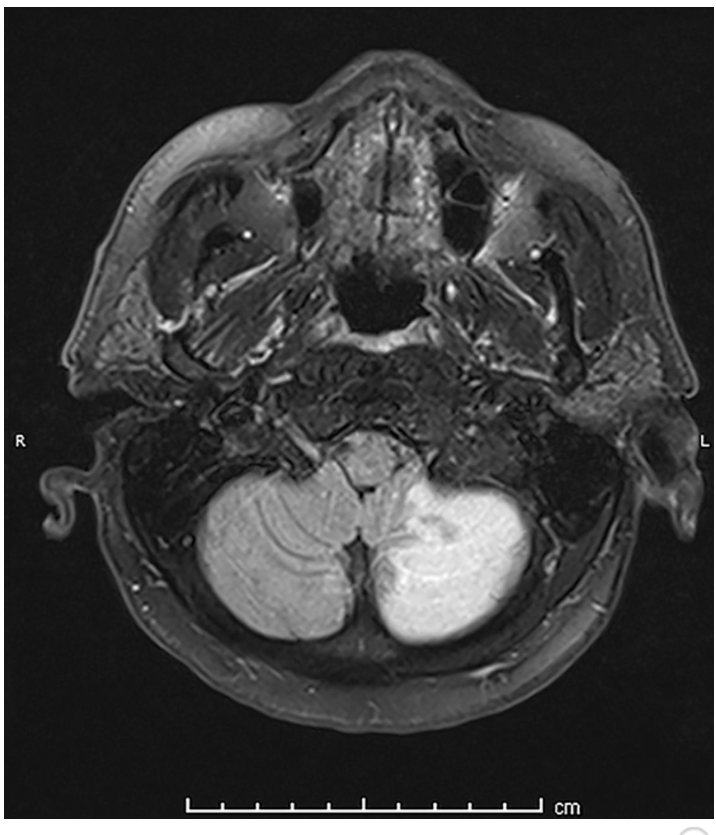
Figure: Brain MRI, fluid-attenuated inversion recovery
Image shows the patient’s infarct, involving the caudal portion of the left cerebellar hemisphere. Area of involvement corresponds to posterior inferior cerebellar artery territory.

Video 1: Rotatory nystagmus toward the left in all directions of gaze but worse on left and upward gaze. Rotatory nystagmus improved in amplitude and frequency with low dose clonazepam. http://movie-usa.

Video 2: Video shows rhythmic contractions of the soft palate.
http://movie-usa.
References
1. Tilikete C, Desestret V. Hypertrophic olivary degeneration and palatal or oculopalatal tremor. Front Neurol 2017;8:302.Google Scholar
2.Borruat FX. Oculopalatal tremor: current concepts and new observations, Curr Opin Neurol 2013;26:67–73.
Neuro-ophthalmology Illustrated Chapter 1 – Examination 6
December 5, 2018 By
Questions:
25. Do metabolic causes of coma usually result in large or small pupils?
26. What is ocular bobbing?
27. What is the likely location of a lesion with ocular bobbing?
28. What is ocular dipping?
Recommended Reading – Ocular myasthenia gravis: an update on diagnosis and treatment
November 29, 2018 By
Recommended Reading – Ocular myasthenia gravis: an update on diagnosis and treatment
Ocular myasthenia gravis: an update on diagnosis and treatment
Elizabeth Fortina, Dean M. Cestaria, and David H. Weinberg
Current Opinion in Ophthalmology. 2018.29:6
Purpose of review
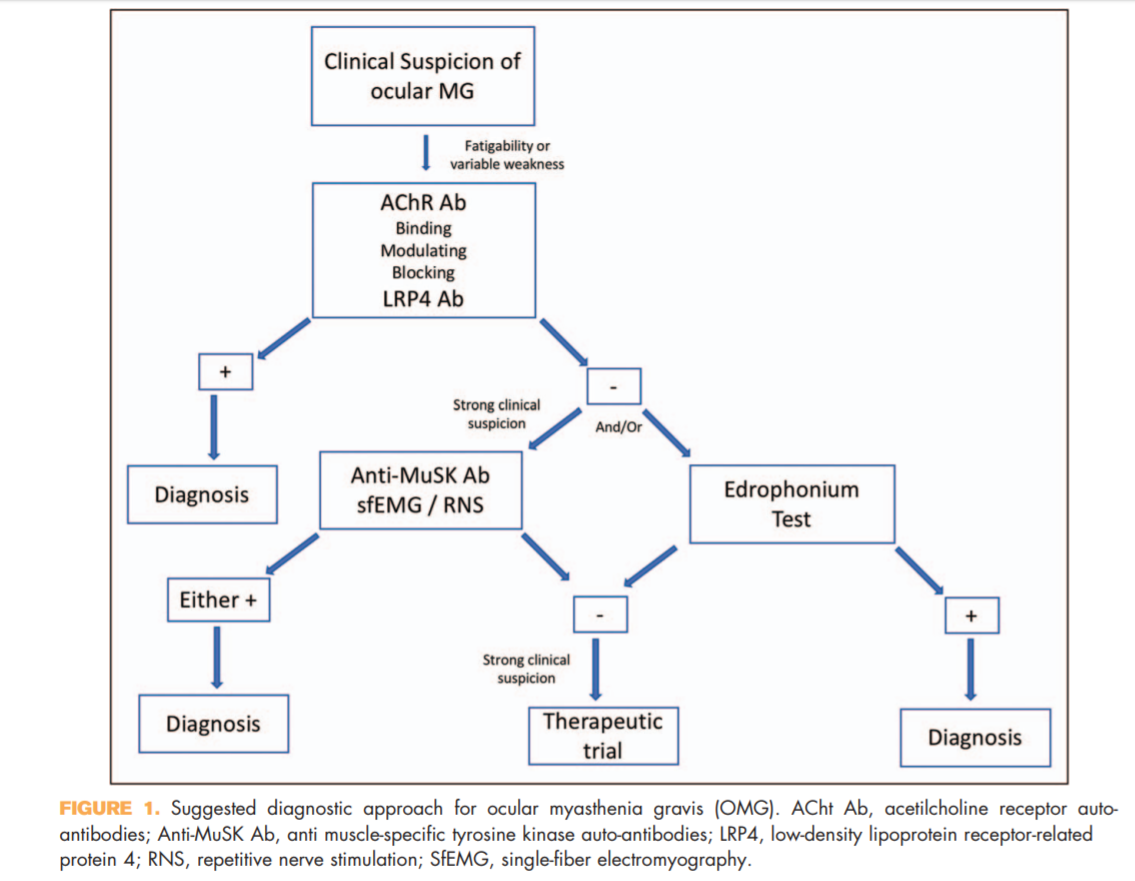
Myasthenia gravis is an autoimmune disease that commonly affects the palpebral and extraocular muscles. Ocular myasthenia gravis (OMG) is a variant of the disease that is confined to the ocular muscles but frequently becomes generalized over time. The diagnosis of OMG is often challenging but both clinical and laboratory findings are helpful in confirming the clinical suspicion. This review provides an update on the diagnostic approach and therapeutic options for OMG.
Recent findings
Antimuscle-specific tyrosine kinase and LDL-related receptor-related protein 4 are newly available serologictesting for myasthenia gravis that can help in increasing the diagnostic sensitivity of OMG. They should be included to the diagnostic algorithm of OMG in appropriate clinical situations.
Summary
OMG remains a primarily clinical diagnosis, but recent advances in laboratory testing can improve the diagnostic accuracy and should be used in appropriate clinical settings. The mainstay of treatment for OMG has not significantly changed over the past years, but the increasing availability of steroid-sparing agents improved the disease control while minimizing steroid-induced complications.
KEY POINTS
● OMG remains a clinical diagnosis, but various laboratory and electrophysiologic testing can help in increasing the diagnostic accuracy.
● Antimuscle-specific tyrosine kinase and LDL-related receptor-related protein 4 antibodies should be included in the diagnostic algorithm of patients suspected to have OMG.
● Therapy should aim at achieving satisfactory symptomatic control while reducing minimizing
Full Text https://drive.google.com/open?id=1ArU1gdYCwKWogLDCr0OcslzGd6egLN8y
Neuro-ophthalmology Illustrated Chapter 1 – Examination 5
November 28, 2018 By
Questions:
21. What are 5 clinical settings where OKN testing may be helpful?
22. Why should OKN testing be done in infants suspected of having the infantile nystagmus syndrome (congenital nystagmus)?
23. Where is the lesion likely to be located in a patient with homonymous hemianopia and symmetric OKN?
24. Where is the lesion likely to be located in a patient with homonymous hemianopia and asymmetric OKN response?
Neuro-ophthalmology Illustrated Chapter 1 – Examination 4
November 21, 2018 By
Questions:
17. Anisocoria more obvious in dim light indicates a sympathetic or parasympathetic lesion?
18. Dilation lag present when the lights are dimmed indicates a sympathetic or parasympathetic lesion?
19. How long after dimming the lights should one wait before checking for dilation lag?
20. Anisocoria more obvious in bright light indicates a sympathetic or parasympathetic lesion?
Neuro-ophthalmology Illustrated Chapter 1 – Examination 3
November 14, 2018 By
Questions:
11. Which 5 features of pupil function should be documented in a neuro-ophthalmic examination?
12. Would a Relative Afferent Pupillary Defect be expected with anisocoria?
13. Does an occipital lobe injury result in a Relative Afferent Pupillary Defect?
14. Does a unilateral optic neuropathy result in a Relative Afferent Pupillary Defect?
15. Can a unilateral optic tract lesion result in a Relative Afferent Pupillary Defect?
16. What anatomic factor explains the Relative Afferent Pupillary Defect with an optic tract lesion?
Recommended Reading – The expanding burden of idiopathic intracranial hypertension
November 7, 2018 By
Recommended Reading – The expanding burden of idiopathic intracranial hypertension
The expanding burden of idiopathic intracranial hypertension
Susan P. Mollan, Magda Aguiar, Felicity Evison, Emma Frew & Alexandra J. Sinclair. Eye (2018)
Free Full Text: https://www.nature.com/articles/s41433-018-0238-5
Abstract
OBJECTIVE: To quantify the hospital burden and health economic impact of idiopathic intracranial hypertension.
METHODS: Hospital Episode Statistics (HES) national data was extracted between 1st January 2002 and 31st December 2016. All those within England with a diagnosis of idiopathic intracranial hypertension were included. Those with secondary causes of raised intracranial pressure such as tumours, hydrocephalus and cerebral venous sinus thrombosis were excluded.
RESULTS: A total of 23,182 new IIH cases were diagnosed. Fifty-two percent resided in the most socially deprived areas (quintiles 1 and 2). Incidence rose between 2002 and 2016 from 2.3 to 4.7 per 100,000 in the general population. Peak incidence occurred in females aged 25 (15.2 per 100,000). 91.6% were treated medically, 7.6% had a cerebrospinal fluid diversion procedure, 0.7% underwent bariatric surgery and 0.1% had optic nerve sheath fenestration. Elective caesarean sections rates were significantly higher in IIH (16%) compared to the general population (9%), p < 0.005. Admission rates rose by 442% between 2002 and 2014, with 38% having repeated admissions in the year following diagnosis. Duration of hospital admission was 2.7 days (8.8 days for those having CSF diversion procedures). Costs rose from £9.2 to £50 million per annum over the study period with costs forecasts of £462 million per annum by 2030.
CONCLUSIONS: IIH incidence is rising (by greater than 100% over the study), highest in areas of social deprivation and mirroring obesity trends. Readmissions rates are high and growing yearly. The escalating population and financial burden of IIH has wide reaching implications for the health care system.
Composite figure.
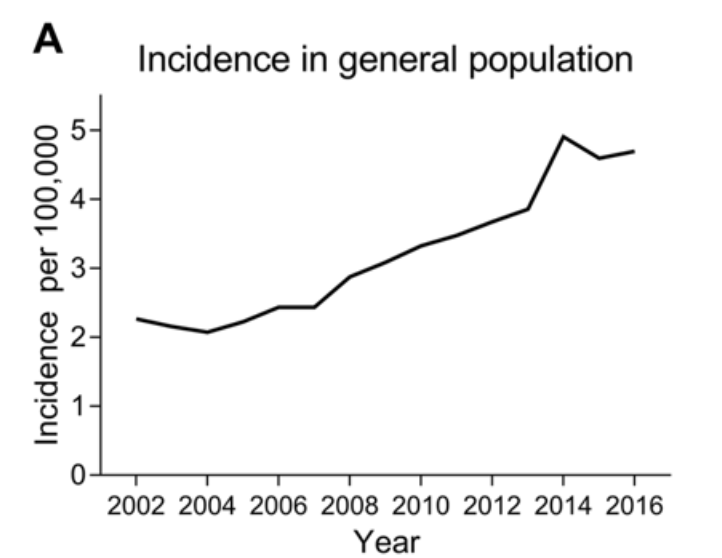
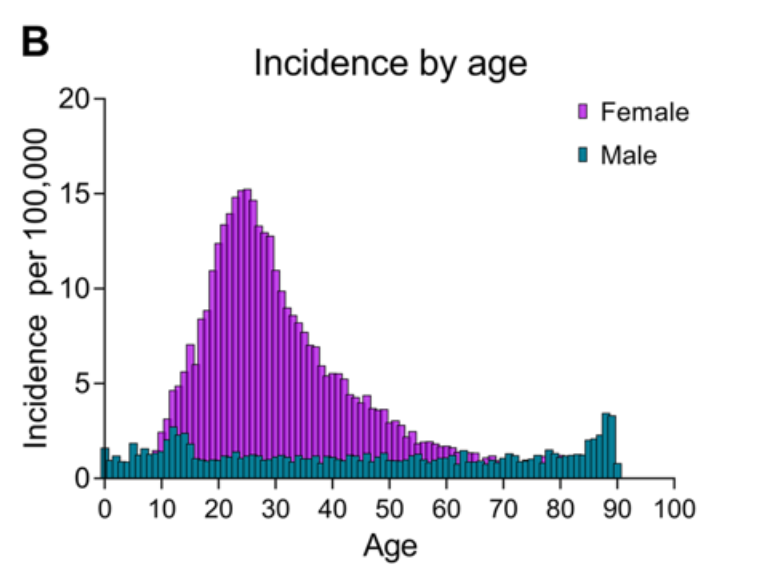
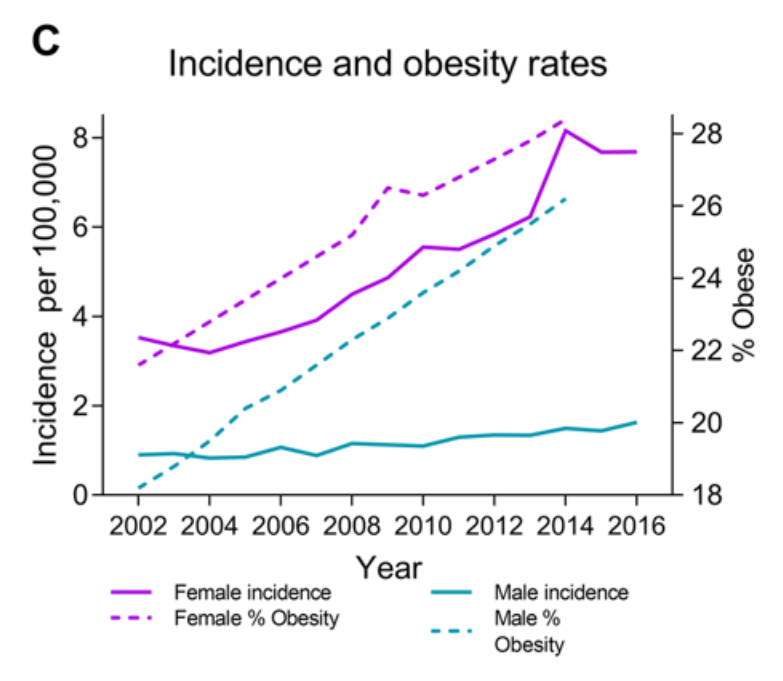
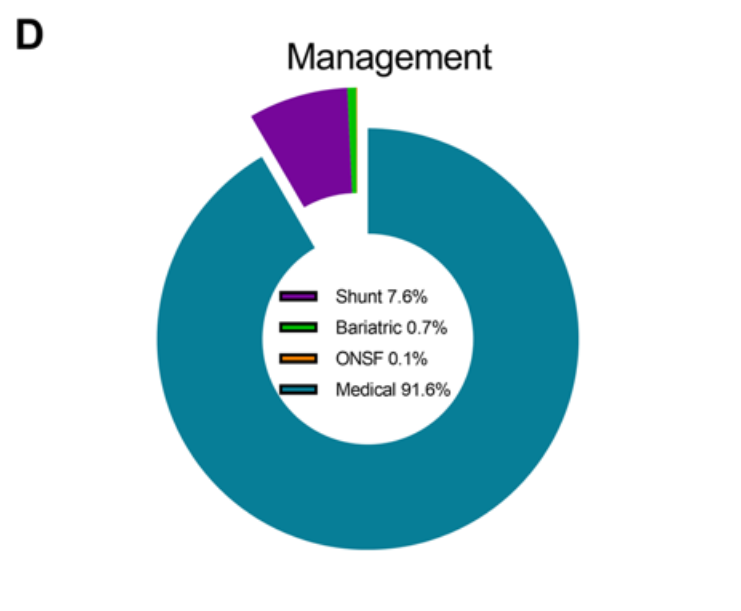
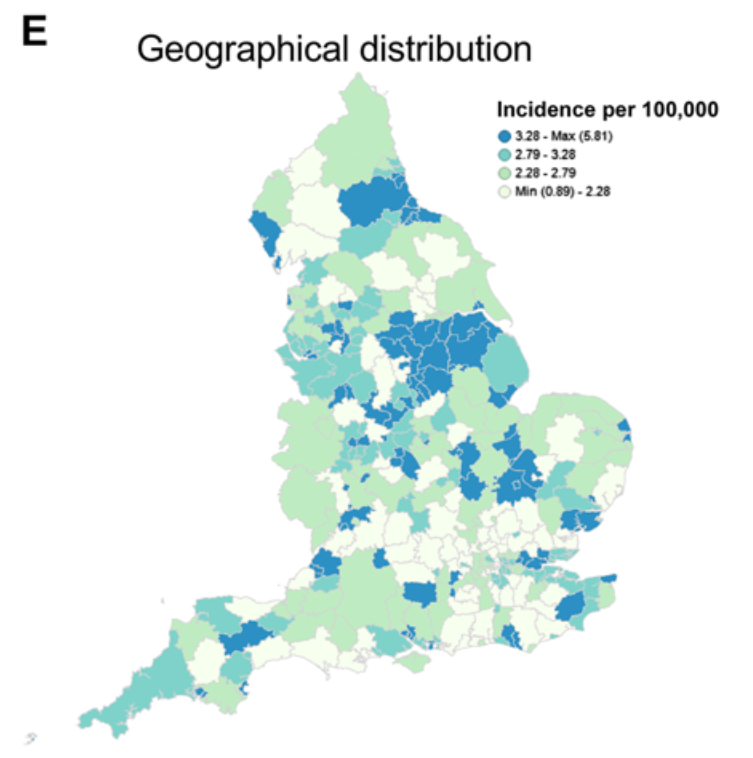
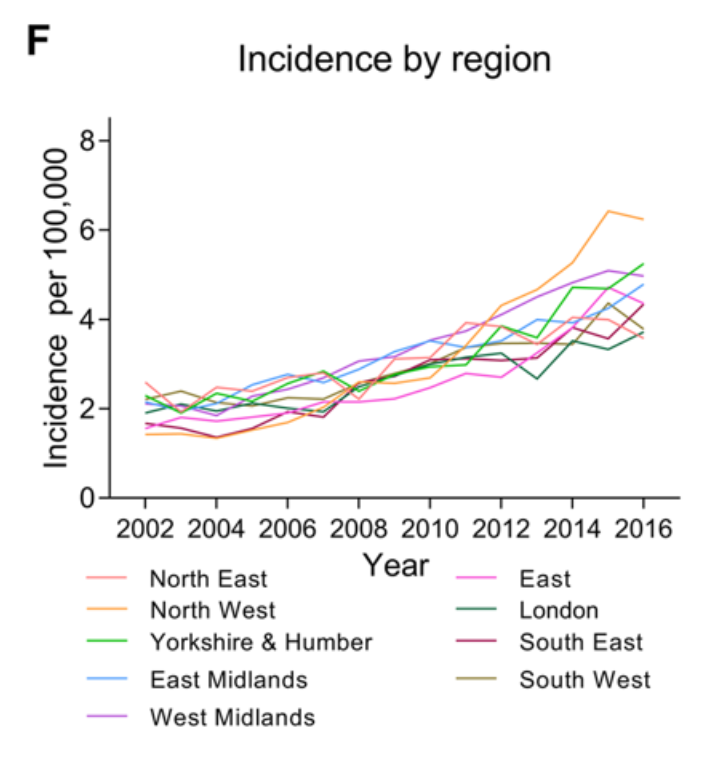
a Incidence in the general population. b Incidence by age and gender. c Annual incidence in females and males and Obesity rates (% obesity per annum (body mass index ≥ 30), age-standardized in 18 years + by gender in the United Kingdom. From World Health organisation http://apps.who.int/gho/data/node.main.A900A?lang=en Accessed 6 Oct 2017. d Management of IIH in the cohort. e Geographical distribution of diagnosed cases of IIH in England. F Distribution of cases by region per annum.
Neuro-ophthalmology Illustrated Chapter 1 – Examination 2
November 7, 2018 By
Questions:
4. For the Photostress Recovery Test, how long does the patient look at a bright light held a few centimeters from the eye?
5 For the Photostress Recovery Test, what is the recovery end point to observe?
6. For the Photostress Recovery Test, what is the normal recovery time?
7. Which conditions prolong the recovery time of the Photostress Recovery Test?
8. What is the normal height of the palpebral fissure?
9. What is the normal Marginal Reflex Distance (MRD1)?
10. How many millimeters is the normal levator function measurement?
Neuro-ophthalmology Illustrated Chapter 1 – Examination 1
October 31, 2018 By
Questions:
1. What is the minimum visual acuity needed to correctly read the control plate on the color vision testing plates?
2. Which is the more sensitive color vision test, Hardy-Rand-Rittler or Ishihara for optic neuropathy?
3. What are the causes of acquired unilateral or bilateral reduced color vision?