Recommended Reading – Teaching Video NeuroImages: Oculopalatal myoclonus
Teaching Video NeuroImages: Oculopalatal myoclonus
A possible consequence of brainstem injury
Neurology. November 27, 2018; 91 (22) RESIDENT & FELLOW SECTION
A 61-year-old man with previous left cerebellar infarct complained of double vision and dizziness several months postinfarct. Infarct is shown in the figure. Examination showed rotatory nystagmus in all directions of gaze, worse on left gaze (video 1). Oral examination showed palatal tremor (video 2). Oculopalatal tremor (OPT) is thought to result from interruption of connections between the red nucleus (midbrain), dentate nucleus (cerebellum), and inferior olive (medulla).1,2 The most common cause is brainstem infarction or hemorrhage,1 but it has also been observed with multiple sclerosis and other inflammatory entities. OPT usually becomes apparent several months after the injury. Treatment may include gabapentin, memantine, benzodiazepines, and valproic acid.
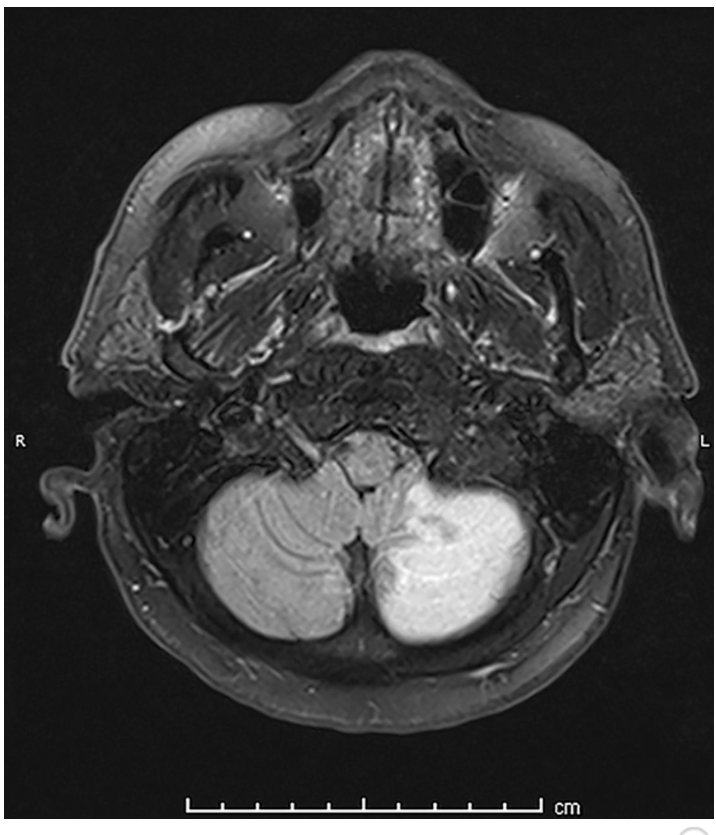
Figure: Brain MRI, fluid-attenuated inversion recovery
Image shows the patient’s infarct, involving the caudal portion of the left cerebellar hemisphere. Area of involvement corresponds to posterior inferior cerebellar artery territory.

Video 1: Rotatory nystagmus toward the left in all directions of gaze but worse on left and upward gaze. Rotatory nystagmus improved in amplitude and frequency with low dose clonazepam. http://movie-usa.

Video 2: Video shows rhythmic contractions of the soft palate.
http://movie-usa.
References
1. Tilikete C, Desestret V. Hypertrophic olivary degeneration and palatal or oculopalatal tremor. Front Neurol 2017;8:302.Google Scholar
2.Borruat FX. Oculopalatal tremor: current concepts and new observations, Curr Opin Neurol 2013;26:67–73.