Questions:
1. What drops should be used to dilate the pupils for examination?
2. How long does dilation with usually last?
3. Why is it always better to dilate both eyes rather than one eye?
4. Is glaucoma a contraindication for pupillary dilation?
5. What are 5 causes of an abnormal red reflex?
6. What are 14 examples of systemic disorders in which examination of the fundus may be abnormal even without visual symptoms?
____________________________________________________
Questions with answers:
1. What drops should be used to dilate the pupils for examination?
To dilate the pupils use a combination of short-acting agents that block parasympathetic transmission (tropicamide) and enhance sympathetic activity (phenylephrine). It also possible to use only one drop.
2. How long does dilation with usually last?
Dilation occurs within 30 minutes and usually resolves within 6 hours.
3. Why is it always better to dilate both eyes rather than one eye?
A unilateral mydriasis is often alarming, whereas most people will not be concerned about bilateral mydriasis if the patient is awake and alert.
4. Is glaucoma a contraindication for pupillary dilation?
Glaucoma is not a contraindication for pupillary dilation. Patients who know they have a diagnosis of angle closure glaucoma and already have been treated with laser to prevent episodes of angle closure from pupillary dilation and can therefore be dilated without risk. Nearly all patients who say they have glaucoma have open angle glaucoma, which does not contraindicate pupillary dilation.
5. What are 5 causes of an abnormal red reflex?
1. cataract
2. severe retinal disorder involving the posterior pole (a large retinal scar and is particularly common with a large retinal detachment)
3. vitreous hemorrhage
4. ocular mass (retinoblastoma, melanoma)
5. strabismus
6. What are 14 examples of systemic disorders in which examination of the fundus may be abnormal even without visual symptoms?
Systemic hypertension
2. Malignant hypertension (hypertensive crisis)
3. Diabetes mellitus
4. Sickle cell disease
5. Human immunodeficiency virus (HIV) infection with low CD4 count
6. Severe thrombocytopenia
7. Endocarditis, septicemia
8. Systemic vasculitis, autoimmune disease
9. Headache
10. Any cause of raised intracranial pressure
11. Intracranial mass
12. Any cause of meningeal process
13. Subarachnoid hemorrhage
14. Stroke
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
2 Funduscopic Examination
The ocular fundus can be viewed directly through the pupil with the help of an ophthalmoscope. Examination of the fundus is essential in cases of visual loss, but it is also helpful in detecting numerous systemic and neurologic disorders.
2.1 What Is Seen with an Ophthalmoscope
▶Fig. 2.1 diagrams what is seen on examination of the fundus with a direct ophthalmoscope.

▶Fig. 2.2 shows a patient being examined with a direct PanOptic (Welsh Allyn, Skaneates Falls, NY) ophthalmoscope, which features a larger field but less magnification than the classic direct ophthalmoscope.

The following make direct ophthalmoscopy easier:
1. Get close to the patient.
2. Use your right eye to look into the patient’s right eye, and use your left eye to look into the patient’s left eye.
3. Find the red reflex and get closer until you see the retina.
4. After focusing on the retina, follow the blood vessels toward the patient’s nose to find the optic nerve.
5. To easily find the macula, ask the patient to look into the light.
6. Dilate the pupils to allow easier examination (▶Fig. 2.3).
It is possible to visualize the optic nerve through an undilated pupil. However, it is technically difficult, and it does not allow examination of the entire fundus. Retinal disorders are missed without pupillary dilation.

Pearls
To view the ocular fundus to the best advantage, the pupils should be dilated. To dilate the pupils use a combination of short-acting agents that block parasympathetic transmission (tropicamide) and enhance sympathetic activity (phenylephrine). It also possible to use only one drop. Dilation occurs within 30 minutes and usually resolves within 6 hours. Long-acting dilating drops (used as cycloplegics), such as cyclopentane-late, homatropine, and atropine, should not be used to view the fundus (the dilation and cycloplegia may last from 12 hours to up to 14 days).
Be sure to alert the patient that driving may be difficult after dilation, especially in bright sunlight. Young patients will have difficulty reading after pharmacologic dilation because of the blockage of accommodation.
It is always better to dilate both eyes rather than one eye (a unilateral mydriasis is often alarming, whereas most people will not be concerned about bilateral mydriasis if the patient is awake and alert). Always document the time of dilation and the drops used. Do not dilate a neurosurgical or unstable patient, because monitoring of the pupils may be important.
Glaucoma is not a contraindication for pupillary dilation. Patients who know they have a diagnosis of angle closure glaucoma will already have been treated with laser to prevent episodes of angle closure from pupillary dilation and can therefore be dilated without risk. Nearly all patients who say they have glaucoma have open angle glaucoma, which does not contraindicate pupillary dilation.
Funduscopic examination includes the optic nerve (specifically, checking for cup-to-disc ratio, edema, and pallor), the retina around the optic nerve, the macula (specifically, checking for color, edema, hemorrhages, exudates, and masses), and arteries and veins (specifically, checking for size, occlusion, and emboli) (▶Fig. 2.4).
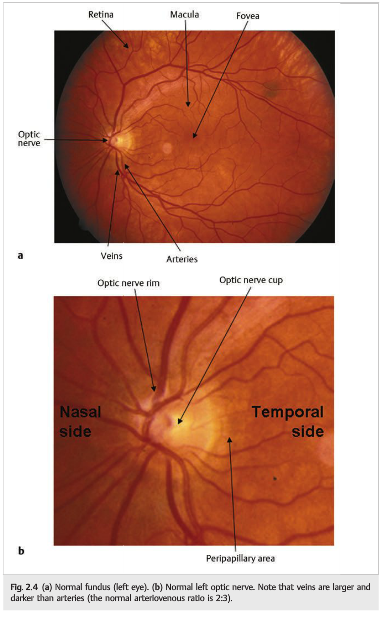
The cup-to-disc ratio (the size of the cup in relation to the size of the disc) should be measured horizontally and vertically (▶Fig. 2.5).

2.1.1 If You Cannot See the Fundus
If you are unable to see the fundus on examination, review the following checklist:
1. Is the ophthalmoscope working? (are the batteries charged?)
2. Is the pupil too small? (Did you forget to dilate the patient’s pupils?)
3. Are you sure you know how to use the ophthalmoscope?
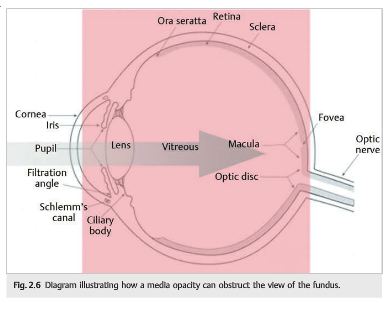
4. Is there something blocking the view (media opacity)? Many ocular disorders—corneal disorders, anterior uveitis or hyphema, cataracts, and vitreous inflammation or hemorrhage—decrease the normal transparency of the ocular media, thereby obstructing the view of the fundus (▶Fig. 2.6). Remember that if you can’t see in, the patient can’t see out.
An easy way to check for media opacity is to look for the red reflex with the ophthalmoscope (compare both eyes):
1. Look through the ophthalmoscope at about 2 feet from the patient’s eye and direct the light straight into the pupil.
2. You should see an orange-red reflex (reflection of the light on the normal orange-red retina) (▶Fig. 2.7). (This is what you observe when a camera flash gives subjects red eyes.)
3. By retroilluminating the cornea and the lens and using “plus” (green numbers)lenses in the direct ophthalmoscope, you can use the red reflex to look for corneal and lens opacities (cataracts) at the bedside (▶Fig. 2.8).


When there is a severe retinal disorder involving the posterior pole, or a vitreous hemorrhage (▶Fig. 2.9), the red reflex can also be abnormal.
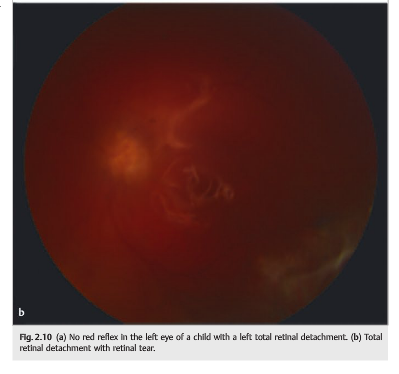
This is particularly common with a large retinal detachment (▶Fig. 2.10), an ocular mass (retinoblastoma, melanoma), and large retinal scars.

2.1.2 If You Have a Clear View of the Fundus
Most causes of monocular central visual loss that are not due to media abnormalities result from disorders of either the optic nerve or the macula. Although more peripheral retinal findings may provide important diagnostic clues, it is primarily disease of the optic nerve or the most central retina that results in loss of central visual function, and many of these disorders can be seen with a direct ophthalmoscope.
Pertinent visible abnormalities include the following (▶Fig. 2.11—2.20):
● Disc edema
● Disc pallor
● Whitening of the inner retinal layers secondary to infarction, as in central and branch retinal artery occlusions
● Hemorrhages and venous dilation in central retinal vein occlusion
● Detachment Of the retina or accumulation of subretinal fluid, as in central serous retinopathy
● Degeneration of the retina, as in macular degeneration
● Abnormalities of the retinal vasculature, including thrombosis and emboli
● Vasculitis with arterial or venous sheathing or exudate deposition, such as may result from infections like syphilis or systemic inflammatory disorders such as sarcoidosis




2.2 Fundus Photography Is Another Way to Examine the Ocular Fundus
Digital photography of the ocular fundus is widely used to examine the optic nerve and the retina. Non Mydriatic cameras allow excellent-quality photographs without pharmacological dilation of the pupils and provide very good views of the posterior pole(optic nerve, macula, and vascular arcades). The photographs can be easily analyzed on a computer, a tablet, or even a smartphone (▶Fig. 2.21); they can also be transmitted electronically for remote consultation (see▶Fig. 1.34).

2.3 When to Examine the Fundus
Examples of systemic and neurologic disorders in which examination of the fundus should be systematic, even in the absence of visual symptoms, include the following:
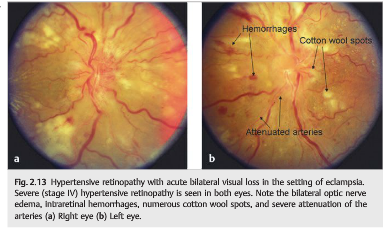
● Systemic hypertension
● Malignant systemic hypertension (hypertensive crisis)
● Diabetes mellitus
● Sickle cell disease
● Human immunodeficiency virus (HIV) infection with low CD4 count
● Severe thrombocytopenia
● Endocarditis, septicemia
● Systemic vasculitis, autoimmune disease
● Headache
● Any cause of raised intracranial pressure
● Intracranial mass
● Any cause of meningeal process
● Subarachnoid hemorrhage
● Stroke
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.