Questions:
4. For the Photostress Recovery Test, how long does the patient look at a bright light held a few centimeters from the eye?
5 For the Photostress Recovery Test, what is the recovery end point to observe?
6. For the Photostress Recovery Test, what is the normal recovery time?
7. Which conditions prolong the recovery time of the Photostress Recovery Test?
8. What is the normal height of the palpebral fissure?
9. What is the normal Marginal Reflex Distance (MRD1)?
10. How many millimeters is the normal levator function measurement?
____________________________________________________
Questions with answers:
4. For the Photostress Recovery Test, how long does the patient look at a bright light held a few centimeters from the eye?
10 seconds
5. For the Photostress Recovery Test, what is the recovery end point to observe?
The endpoint is the number of seconds for visual acuity to return to within one line of the best corrected visual acuity.
6. For the Photostress Recovery Test, what is the normal recovery time?
Less than 30 seconds
7. Which conditions prolong the recovery time of the Photostress Recovery Test?
Maculopathies – NOT Optic neuropathies
8. What is the normal height of the palpebral fissure?
9-12 mm
9. What is the normal Marginal Reflex Distance (MRD1)?
4- 5 mm
10. How many millimeters is the normal levator function measurement?
>12 mm (13-17 mm)
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
1.4 Photostress Recovery Test
Photostress recovery is used to differentiate between macular disease and optic neuropathy. The principle underlying this test is that recovery of retinal sensitivity following exposure to a bright light is based on regeneration of visual pigments that were bleached during exposure to light. A delay in this process occurs in diseases affecting the photoreceptors and is independent of the neural pathways.
Each eye is tested separately:
1. Measure the best corrected visual acuity in each eye.
2. Have the patient look directly into a bright light held a few centimeters from the eye for 10 seconds.
3. Record the time taken for the visual acuity to return to within one line of the best corrected visual acuity. Most normal patients will have a recovery time of less than 30 seconds, which is symmetric between the two eyes. Macular diseases (but not optic neuropathies) often cause a prolongation in the photostress recovery time. This is particularly useful for unilateral or subtle macular diseases.
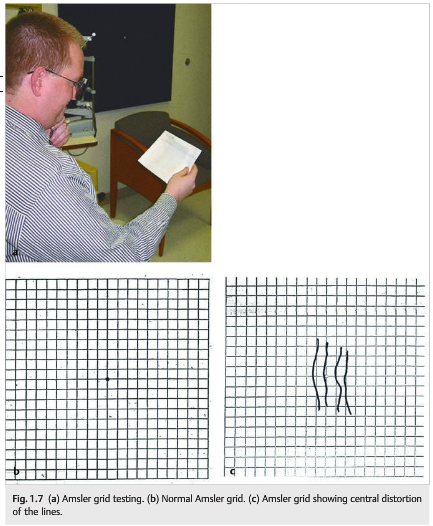
1.5 Amsler Grid
The Amsler grid is very useful in detecting macular abnormalities as a cause of visual loss (▶Fig. 1.7a).
Each eye is tested separately, and the patient is asked to fixate on a central point in a square grid of lines and to draw any area in which the lines disappear or are broken, warped, double, or curved.
Patients with maculopathy often see the straight lines as curved (metamorphopsia).
1.6 Stereo Vision
Stereo vision is tested on a specific book (Titmus test) with both eyes open and polarized glasses placed on the patient’s reading corrective lenses. This book shows animals and circles that are seen in stereo with the polarized glasses (▶Fig. 1.8)
Stereopsis requires binocular vision. Therefore, the presence of stereopsis indicates at least some vision in each eye. This test is very helpful when nonorganic visual loss is suspected.
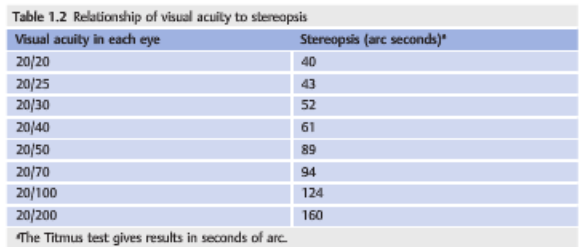
Stereopsis can be quantified and correlated with visual acuity (▶Table 1.2).

1.7 Eyelid Examination
An eyelid examination includes evaluation of the following:
● Position of the eyelids○ Ptosis (droopy eyelid)○ Retraction
● Lid function
● Swelling
● Mass
In normal individuals, the upper lid covers the superior 1 to 2mm of the iris, while the lower lid just reaches the inferior aspect of the iris (▶Fig. 1.9). Examination of the eyelids (▶Fig. 1.10 and ▶Fig. 1.11) includes measurements of the following:
● Palpebral fissure: distance between the upper and lower eyelid in vertical alignment with the center of the pupil (normal 9–12mm)
● Margin reflex distance (normal 4–5mm)○ Marginal reflex distance-1 (MRD-1): distance between the center of the pupillary light reflex and the upper eyelid margin with the eye in primary gaze○ Marginal reflex distance-2 (MRD-2): distance between the center of the pupillary light reflex and the lower eyelid margin with the eye in primary gaze
● Levator function: distance the eyelid travels from downgaze to upgaze while the frontalis muscle is held inactive at the brow. A measurement of greater than 10mm is considered excellent, whereas 0 to 5mm is considered poor.
For more information on disorders of the eyelid, see Chapter 17.
1.8 Orbital Examination
An orbital examination includes the following:
● Inspection of the patient’s external appearance:
○ Orbital deformations
– Hypo- or hypertropia of the globes
○ Abnormal position of the eyes within the orbits
– Proptosis (eye bulging out of the orbit)
– Enophthalmos (eye sinking into the orbit)
○ Periorbital soft tissues
– Swelling
– Redness
– Hematoma
– Mass
● Palpation of the orbital rims
● Resistance to retropulsion of the eyes
● Auscultation of the orbital contents (for a bruit)
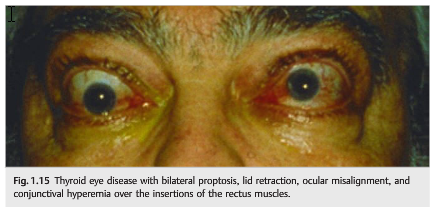
Proptosis can be measured with the Hertel exophthalmometer (▶Fig. 1.12) and on neuroimaging (▶Fig. 1.13). Deformations (▶Fig. 1.14) and disease (▶Fig. 1.15) cause various orbital syndromes. For more information on orbital syndromes, see Chapter 14.



Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.