Recommended Reading – Abnormal Eye Movements in Paraneoplastic Syndromes
Opsoclonus (Ri antibodies)
931-1 Paraneoplastic Opsoclonus http://www.kaltura.com/index.php/extwidget/preview/partner_id/797802/uiconf_id/27472092/entry_id/0_47rqop2q/embed/auto?
Title: Paraneoplastic Opsoclonus Subject: Opsoclonus; Ocular Flutter; Oscillopsia; Saccadic Oscillations; Paraneoplastic Cerebellar Syndrome; Adenocarcinoma of the Breast; Anti-Ri Antibody; Paraneoplastic Opsoclonus; Paraneoplastic Ocular Flutter; Saccadomania Description: This patient is the index case of the Anti-Ri antibody, published in Annals of Neurology in 1988 (4). The Anti-Ri antibody is recognized to be a paraneoplastic marker in patients with breast and gynecological malignancies (10). The history of this case is particularly important because she was initially misdiagnosed as a case of acute labyrinthitis.
Ocular flutter (Ri antibodies)
https://www.aao.org/annual-meeting-video/ocular-flutter
Rod Foroozan. AAO Subspecialty Day 2011: Neuro-Ophthalmology (AAO sign-in may be required)
In this case discussion from Neuro-Ophthalmology Subspecialty Day 2011, Dr. Rod Foroozan presents a case of ocular flutter, a rare disorder characterized by back-to-back saccades. The abnormal ocular oscillations are believed to result from dysfunction of the pause/burst cells, which govern saccade generation, in the pons. The most common causes can be categorized as inflammatory, infectious or paraneoplastic. Most patients with an infectious cause show spontaneous improvement weeks to months after the onset of symptoms.
Cerebellar degeneration (Yo antibodies)
Paraneoplastic Cerebellar Degeneration. Hain TC. 2016
Downbeat Nystagmus anti-YO paraneoplastic cerebellar degeneration
Downbeat Nystagmus in paraneoplastic cerebellar degeneration in left gaze
Downbeat Nystagmus in paraneoplastic cerebellar degeneration increased with convergence
Website https://www.dizziness-and-balance.com/disorders/central/cerebellar/pcd.htm
Downbeat Nystagmus https://www.youtube.com/watch?v=FrlsK4MF3Ao
Downbeat Nystagmus is a “central” or brain-related abnormal eye movement that could have no identifiable cause, but it might suggest abnormalities in the brainstem or cerebellum region of the central nervous system, is often seen in cerebellar degeneration syndromes, vitamin B12 or B1 (thiamine) deficiency, magnesium deficiency, and may be part of a paraneoplastic syndrome.
Elliptical Nystagmus and Oscillopsia
Teaching Video NeuroImages: P/Q-type voltage-gated calcium channel–associated paraneoplastic elliptical nystagmus. Mistry EA, Lee AG, Lai EC. Neurology. 2016.
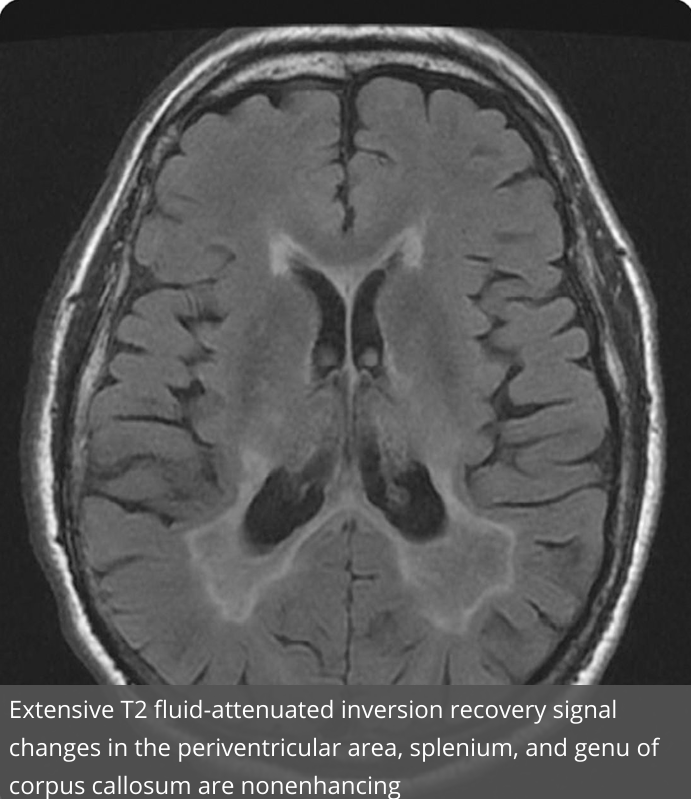
A 71-year-old chronic smoker had an 11-month history of monocular followed by binocular elliptical nystagmus and oscillopsia (video at Neurology.org). MRI brain showed extensive periventricular T2 signal changes (figure) and CSF showed elevated protein to 102 mg/dL. CSF and serum paraneoplastic panel revealed elevated serum titers of anti-P/Q-type voltage-gated calcium channel (VGCC) and anti-neuronal-type voltage-gated potassium channel antibodies. An underlying malignancy was not found after an extensive investigation. The patient was treated with carbamazepine for symptomatic control, followed by high-dose IV methylprednisolone, resulting in moderate improvement. Anti-VGCC antibodies have been implicated in paraneoplastic nystagmus and small cell lung cancer is the most common associated malignancy.1,2
Paraneoplastic upbeat nystagmus.
Wray SH, Martinez-Hernandez E, Dalmau J, Maheshwari A, Chen A, King S, Bishop Pitman M, Leigh RJ. Neurology.2011:16;77(7):691-3.
…During attempted fixation of a far target, she had prominent UBN, lid nystagmus, and saccadic intrusions (video on the Neurology® Web site at www.neurology.org). UBN suppressed during near viewing and showed marked dependency on head position, upbeat when erect, absent when supine, reduced when prone, and beating away from the ground (apogeotropic) when lying on either side.
A CT-guided core biopsy revealed a pancreatic endocrine neoplasm.
Paraneoplastic antibody testing, including anti-Ri, Anti-Yo, anti-Hu, anti-Ma1 and Ma2, anti-ZiC4, and anti-CV2, was positive for anti-Hu antibodies at a titer of 1/15,360. The tumor showed robust reactivity with a monoclonal antibody against Hu confirming the expression of this antigen (figure, A and B). Analysis of patient’s serum and CSF for antibodies against the neuropil of brain, brainstem, and cerebellum (usually indicating a cell membrane or cell surface autoantigen) showed both samples had reactivity with the nuclei of neurons (Hu antigen) as well as with an unknown antigen expressed in the neuropil of brain.
Figure

Expression of Hu antigen by the patient’s tumor, and demonstration of an antibody against a neuronal cell surface antigen
The tumor shows intense reactivity with a mouse monoclonal antibody against human Hu (Molecular Probes; Eugene, OR; Cat# A-21271) used at dilution 1:50 (A).
As a contrast, the tumor does not show reactivity with normal mouse immunoglobulin G used at the same dilution (control section, B).
The immunostaining was performed using the avidin-biotin-peroxidase method followed by hematoxylin counterstaining (×200). Using cultures of dissociated rat hippocampal neurons patient’s serum (diluted 1:100) shows reactivity with the neuronal cell surface (C). The immunolabeling was done using live, not permeabilized neurons, as reported.7
Full-Text https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3159092/
Paraneoplastic disorders may also cause slow saccades and limited vertical movements (Hu, Ma/Ta antibodies).
A recent review: Paraneoplastic Neurologic Syndromes. Rosenfeld MR & Josep Dalmau J. Neurol Clin 36 (2018) 675–685