Questions:
1. What is an orbital syndrome?
2. What are the common features of the orbital syndromes?
3. What are 5 categories of acute or subacute orbital syndromes?
4. What is the most cause of unilateral or bilateral proptosis?
5. What should be suspected if there is proptosis with globe displacement?
6. What tumor is classically associated with fat atrophy and enophthalmos?
7. Why do patients with an orbital syndrome need to be evaluated urgently?
8. What imaging tests are appropriate for orbital syndromes?
9. Do brain CT and MRI scans often miss orbital processes?
10.Is orbital biopsy often necessary?
Neuro-ophthalmology Illustrated Chapter 14 – Orbital Syndromes
March 11, 2020 By
Neuro-ophthalmology questions of the week: NOI19 -Diagnosis of Headache and Facial Pain
September 19, 2018 By
Questions:
1. What 3 types of symptoms can a typical migraine aura have?
2. What is the longest duration of a typical migraine aura?
3. Does a typical migraine aura develop gradually?
4. Characterize the most common type of typical migraine aura?
5. At what point in a migraine with aura attack should vasoconstrictive treatments used to abort the attack be administered (e.g. ergotamine and triptans)?
6. What are the 2 categories of trigeminal neuralgia (tic douloureux)?
7. What differentiates classic from symptomatic trigeminal neuralgia?
8. Name several triggers for trigeminal neuralgia?
9. For Classic Trigeminal Neuralgia, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment?
10. For Symptomatic Trigeminal Neuralgia, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment?
11. For Cluster (Histamine) Headache, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment?
12. For Episodic or Chronic Paroxysmal Hemicrania, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment?
13. For SUNCT Syndrome (Short-lasting, Unilateral, Neuralgiform headache attacks with Conjunctival injection and Tearing), what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment?
14. For Hemicrania Continua, what are the:
1. Age range
2. Gender ratio
3. Location of pain
4. Type of pain
5. Duration of pain
6. Temporal pain profile
7. Associated signs
8. Interictal exam
9. Treatment?
15. What should be measured in all patients with headache?
16. What must be ruled-out in all patients with headache?
17. What must be measured in all patients with recurrent, unilateral pain localized around the eye?
18. What lab tests should be done in all patients over age 50 with any headache or facial pain?
19. What should be considered and done when a patient presents with a thunderclap headache?
Recommended Reading – Abnormal Facial & Ocular Movement Videos
September 12, 2018 By
Recommended Reading – Abnormal Facial & Ocular Movement Videos
Short videos of abnormal facial and ocular movement seen in Dr. C.N. Chua’s clinic.
Ophthalmology Videos page 1 http://www.mrcophth.com/vidoes.html
Ophthalmology Videos page 2 http://www.mrcophth.com/videos2.html
From: Success in MRCOphth by Dr. C.N. Chua http://www.mrcophth.com/chua1.html
Neuro-ophthalmology questions of the week: NOI17-Disorders of the Eyelid 2
September 12, 2018 By
Questions:
16. What is apraxia of eyelid opening?
17. What is thought to cause apraxia of eyelid opening?
18. Apraxia of eyelid is associated with what 4 conditions?
19. What should be ruled out in all cases of ptosis?
20. What are 8 causes of pseudoptosis?
21. What does a show of sclera between the upper eyelid and limbus suggest?
22. What are the 3 categories of eyelid retraction?
23. What are the 3 most common causes of lid retraction?
24. What are 5 causes of mechanical lid retraction?
25. What are 2 causes of myogenic lid retraction?
26. What are 6 causes of neurogenic lid retraction?
27. What may patients with a peripheral facial palsy ultimately develop?
28. What should be suspected in all patients with hemifacial spasm?
29. What test should be done in all patients with hemifacial spasm?
30. What are 4 causes of blepharospasm?
31. A patient has blepharospasm accompanied by dystonic movements of the lower face or neck. What is the diagnosis?
32. Is eyelid pain to be expected in a patient with blepharospasm?
33. How is a patient with blepharospasm likely to describe their eyelid pain?
34. What is the treatment of choice in patients with chronic blepharospasm?
35. What is the treatment of choice in patients with hemifacial spasm?
36. What is the mechanism of action of botulinum toxin injections?
37. Does botulinum toxin injection relieve the crampy pain of a patient with blepharospasm?
Recommended Reading – 1. A ripping roller coaster ride & 2. Stroke
September 5, 2018 By
Recommended Reading – 1. A ripping roller coaster ride & 2. Stroke Due To Extracranial Internal Carotid Artery Dissection After Roller Coaster Rides In A 4-Year-Old Boy
A ripping roller coaster ride
David J. Blacker, Eelco F.M. Wijdicks
Neurology. 2003
NEUROIMAGES
ARTICLE
A 41-year-old woman presented with a right frontotemporal headache and drooping of the right eye. The previous day she rode a violent roller coaster ride twice (figure, left panel) and recalled vigorous jerking of her neck. Examination revealed a right Horner syndrome (figure, middle panel) with ptosis, meiosis, and no anhidrosis. Magnetic resonance angiography (figure, right panel) confirmed the diagnosis of right internal carotid artery dissection.
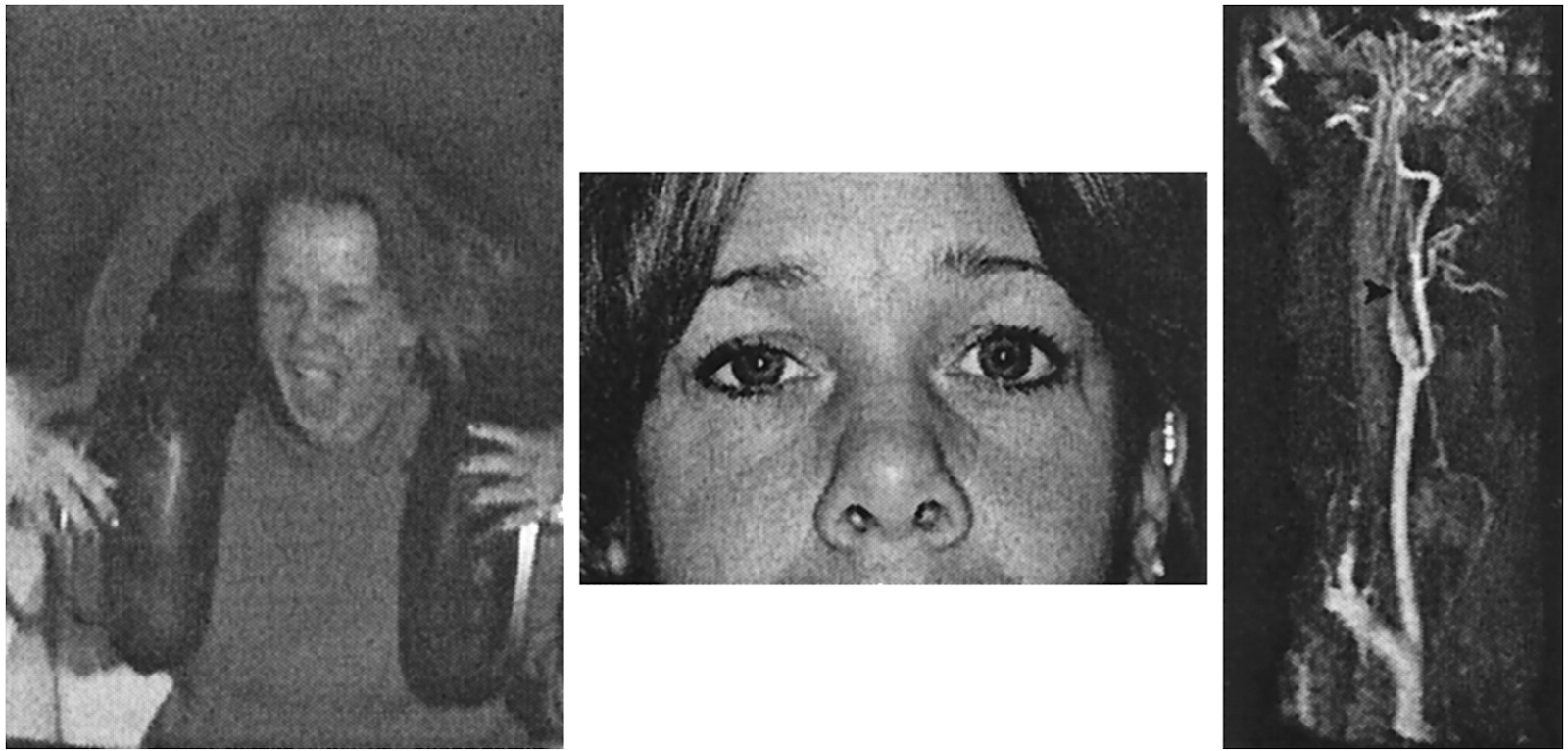
Figure. (A) The patient on the roller coaster ride. (B) Right Horner syndrome. (C) Magnetic resonance angiography confirmed the diagnosis of right internal carotid artery dissection.
Several other cases of carotid dissection have been reported related to amusement park equipment.
1 Roller coaster rides can generate force in excess of 4 “Gs,”1 which in combination with neck movements could potentially rip the carotid intima. Distension of the injured arterial wall compresses the adjacent sympathetic fibers,2 resulting in a Horner syndrome, which is typically without anhidrosis, in lesions above the bifurcation, where the fibers supplying the face leave to traverse with the external carotid artery.
References:
1. Braksiek R, Roberts D. Amusement park injuries and deaths. Ann Emerg Med . 2002; 39: 65–72.
2. Mokri B, Sundt T, Houser W, Piepgras D. Spontaneous dissection of the cervical internal carotid artery. Ann Neurol . 1986; 19: 126–138.
______________________________
Stroke Due To Extracranial Internal Carotid Artery Dissection After Roller Coaster Rides In A 4-Year-Old Boy
Amre Npuh, Daniel Vela-Duarte, Thomas Grobelny, George Hoganson, David Pasquale, Jose Biller.
Neurology. 2014; 82 (10 Supplement)
Abstract
OBJECTIVE: To describe the unusual association of stroke due to an extracranial right internal carotid artery (ICA) dissection following roller-coaster rides in a 4-year old boy. BACKGROUND: Strokes in children should prompt thorough investigations. Strokes associated with roller-coaster rides are unusual.
DESIGN/METHODS: A previously healthy 4-year-old boy frequented many roller coasters with his parents while on vacation at an out of state amusement park. On the flight home the following day, his parents noticed a left facial droop. Upon landing, he was unable to walk due to left sided weakness, prompting immediate evaluation. Magnetic resonance imaging (MRI) of the brain showed an acute right middle cerebral artery (MCA) territory infarction. Magnetic resonance angiography (MRA) showed right M1CA occlusion. Catheter cerebral angiogram performed one week later demonstrated an extracranial right ICA dissection. Transthoracic echocardiogram, extensive hypercoagulable panel, serum autoimmune and inflammatory markers and cerebrospinal fluid (CSF) analysis were unremarkable. Dermatoloical evaluation showed no evidence of connective tissue disease. He received low-dose aspirin.
RESULTS: Neurological function remained stable during his hospital stay, and on a 3 month follow-up he exhibited only mild residual left spastic hemiparesis.
CONCLUSIONS: To our knowledge this is the youngest patient with stroke secondary to ICA dissection following roller-coaster rides. Although the exact mechanism of injury leading to ICA dissection in the setting of sudden linear acceleration, deceleration and rotational forces such as those experienced while riding a roller coaster is not fully understood, these injuries have been attributed to brief sustained excessive gravitational forces likely augmented among predisposed individuals. Children may be at higher risk due to the immature anatomy of their cervical spine. Alterations to roller coaster ride dynamics and use of head restraints may be a reasonable first approach to lower this potential, albeit unusual risk.
Recommended Reading – VIDEO NEUROIMAGES – Bilateral Marcus Gunn jaw-winking syndrome
September 5, 2018 By
Recommended Reading – VIDEO NEUROIMAGES – Bilateral Marcus Gunn jaw-winking syndrome
Deepa Kannaditharayil, Howard Geyer, Henry Hasson, Steven Herskovitz
Neurology. 2015; 84 (10)
ARTICLE
A 10-year-old boy presented with an alternating elevation of his eyelids upon chewing, present since birth (video on the Neurology® Web site at http://www.neurology.org). Examination showed mild left ptosis but no ophthalmoparesis. This represents Marcus Gunn jaw-winking syndrome (MGJWS), also called trigemino-oculomotor synkinesis or pterygoid-levator synkinesis. It likely results from aberrant connections in the midbrain between the trigeminal mesencephalic nucleus and oculomotor nucleus, although others have postulated connections between the mandibular division of trigeminal nerve innervating lateral pterygoid and the superior division of oculomotor nerve innervating levator palpebrae superioris. MGJWS occurs in 2%–13% of patients with congenital ptosis.1 It is usually unilateral but rarely presents bilaterally.2
Video https://www.youtube.com/watch?v=_m6HAys9cdQ
References:
1. Demirci H, Frueh BR, Nelson CC. Marcus Gunn jaw-winking synkinesis: clinical features and management. Ophthalmology 2010;117:1447–1452.
2. Shah AD, Kumar AB, Kothari K. Bilateral Marcus Gunn jaw-winking synkinesis with monocular elevation deficiency: a case report and literature review. Int Ophthalmol 2012;32:199–201.
Neuro-ophthalmology questions of the week: NOI17-Disorders of the Eyelid 1
September 5, 2018 By
Questions:
1. What are 10 causes of ptosis at birth?
2. What are the 4 categories of acquired unilateral or bilateral ptosis?
3. What are 5 types of acquired mechanical ptosis?
4. What are 4 conditions that cause acquired myogenic ptosis?
5. What are 2 causes of an acquired disorder of neuromuscular transmission?
6. What are 3 conditions that cause acquired neurogenic ptosis?
7. Is aponeurotic ptosis usually unilateral or bilateral?
8. What upper eyelid exam findings are likely to be present with aponeurotic ptosis?
9. What is the most common condition causing acquired ptosis in patients over age 50?
10. What usually causes acquired ptosis in young patients?
11. In addition to measuring eyelid positions and levator function, what 2 exam techniques should be performed in all patients with ptosis?
12. What condition must be ruled out in all patients with presumed myogenic ptosis?
13. In Horner syndrome, what is the cause of ptosis?
14. What happens to the ptosis from Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
15. What happens to the pupils in Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
Recommended Reading – IMAGES IN CLINICAL MEDICINE Orbital Varix
August 1, 2018 By
Recommended Reading – IMAGES IN CLINICAL MEDICINE Orbital Varix
Kiang L, Kahana A. N Engl J Med 2015; 372:e9v
A 63-year-old man was referred to our clinic with a 13-year history of intermittent vision loss, binocular diplopia, and blepharoptosis of the left eye during bending or straining that had worsened over the previous year. Other than uneventful cataract surgery, the patient had no clinically significant ocular history, and prior computed tomographic (CT) scans of the head and orbit did not identify any abnormality. An orbital vascular anomaly was suspected. A CT scan of the head was obtained while the patient performed the Valsalva maneuver, revealing the expansile orbital mass. On presentation to us, the patient’s visual acuity was 20/20 in the right eye and 20/50 in the left eye, with a relative afferent pupillary defect in the left eye. There was no proptosis on examination (Panel A).

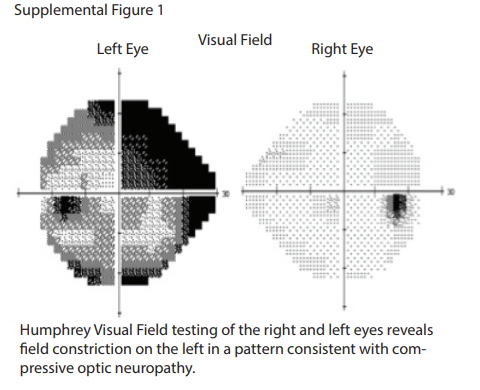
Visual-field testing revealed severe constriction.
A Valsalva maneuver induced 6 mm of proptosis in the left eye, with anterior superior globe displacement and blepharoptosis (Panel B, and video).


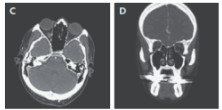
Proptosis quickly reversed on relaxation. CT of the orbit while the patient waw at at rest was unremarkable (Panels C and D show the axial and coronal views, respectively),
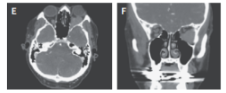
but a Valsalva maneuver revealed an orbital mass causing anterior superior globe displacement (Panels E and F).
An orbital angiogram confirmed the presence of an expansile orbital mass (Fig. 2 in the Supplementary Appendix).
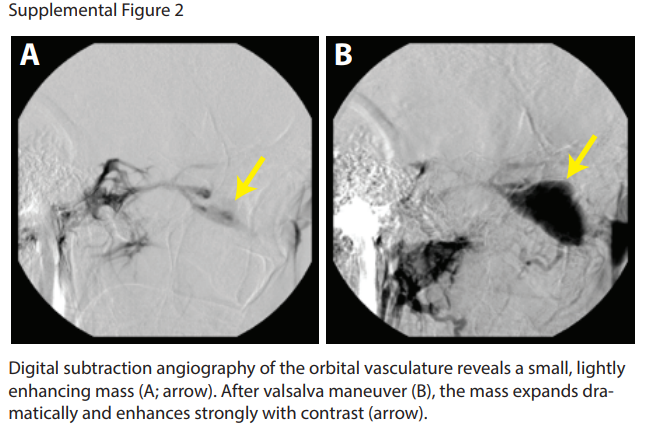
Although the differential diagnosis of an orbital mass is broad and includes lymphoma, metastatic tumors, and inflammatory masses, the clinical findings and imaging studies in this patient were pathognomonic of an orbital vascular anomaly and were most consistent with a distensible venous anomaly (i.e., varix). In the confines of the orbit, an expansile mass can cause intermittent orbital compartment syndrome and compressive optic neuropathy. The patient underwent successful endovascular and transorbital sclerosing treatment. The postoperative visual acuity was 20/30 in the left eye, with a stable visual field.
Neuro-ophthalmology questions of the week: NOI15-Cavernous Sinus and Orbital Vascular Disorders 4
August 1, 2018 By
Questions:
18. What is the cause of “orbital varices”?
19. What should be considered when a crying infant eye bulges?
Recommended Reading Cavernous Sinus Thrombosis
July 25, 2018 By
From: MRI in the Evaluation of Acute Visual Syndromes.
Mukhi SV, Lincoln CM. Topics in Magnetic Resonance Imaging 24 (6):309-24. 2015
https://drive.google.com/open?id=1ayqCxDRn0E_Own4NkKoWbC2zqvfAc2X8
The prevalent use of antibiotics has decreased the overall incidence of CST. CST still carries significant mortality, commonly reported as approximately 30%, with more than 50% of the cases resulting in morbidity secondary to cranial neuropathies. CST is subclassified as aseptic or infectious in etiology. Aseptic causes include surgery or trauma. Infectious CST is typically a complication of a facial, orbital, odontogenic, or paranasal sinus infection. Sinusitis is the most common cause of CST, whereas odontogenic sources have been reported in up to 10% of the cases.3,33–39
The CS is a paired structure on either side of the sella, pituitary gland, and sphenoid sinus. It is composed of two layers of dura that are split to create a septate venous channel. The internal carotid artery (ICA) is the most medial structure and cranial nerves III, IV, and first and second branches of cranial nerve V are located in the lateral wall of the dura. Cranial nerve VI courses at the medial aspect of the ICA. Anteriorly, the CS is bordered by the SOF and OA. The posterior margin of the CS is immediately lateral to the dorsum sella and bordered by Meckel cave medially and the petrous apex posteroinferiorly.33,40,41
CST most commonly occurs secondary to the spread of infection by emissary veins as well as by direct extension. Emissary veins throughout the skull base are valve less and have bidirectional flow, accounting for the ease of contiguous spread.41 Spread of infection also occurs by the propagation of thrombus and/or septic embolism. It is postulated that bacteria stimulate the formation of thrombus by the release of a procoagulant substance and through toxins that cause tissue damage.38 In otitis media, infection spreads via the sigmoid sinus and along the internal carotid artery plexus. Staphylococcus aureus (70%) and Streptococcus sp (22%) are the important organisms responsible for infection of the CS. In patients with uncontrolled diabetes and immunocompromise, fungal infection can also be responsible, particularly mucormycosis.38,41
Tuberculosis has also been reported to cause both unilateral and bilateral CST; cavernous sinus tuberculoma may occur in the absence of pulmonary findings. Lymphomatous infiltration of the CS has been reported in both pediatric and adult patients.4
CST typically presents with orbital swelling, proptosis, chemosis, fever, and ophthalmoplegia. Visual impairment in CST has been reported in 7% to 22% of the cases, with blindness reported in 8% to 15% of the cases. As the disease progresses, decreased light perception and visual loss ensue. In a case report by Chen et al, CST-induced blindness suggested involvement of the bilateral retina and optic nerves. The postulated mechanisms accounting for visual impairment and blindness in CST include venous infarction of the retina and retinal ischemia caused by occlusion of either an ophthalmic artery branch or the central retinal artery, or by mechanical pressure at the OA.39
Chemosis, periorbital edema, and proptosis have been attributed to venous congestion.38 Papilledema as a result of raised intracranial pressure from a CST has been described as well.42 Palsies of III, IV, and VI cranial nerves secondary to compression result in impaired EOM motility. Intracranial extension of infection may result in meningitis, encephalitis, brain abscess, pituitary infection, epidural and subdural empyema, and coma/death.33,38,42
MRI is the radiologic examination of choice, and the CS should be imaged in its entirety. MRI demonstrates the contents of the CSs more effectively compared with CT.40 Imaging protocols should extend from the OA to the prepontine cistern. Routine T2, fluid-attenuated inversion recovery, and pre- and post-contrast T1 weighted images of the entire brain should be included. Postcontrast T1 weighted, 3-mm thick images should be obtained in the axial and coronal planes with at least one plane imaged utilizing a fat-saturation technique. Thin-section, postcontrast axial images may be acquired by three-dimensional spoiled gradient techniques. In addition, thin-section, three-dimensional, heavily T2 weighted images allow visualization of individual cranial nerves in the CS and adjacent cisterns.43 Pula et al describe the use of three-dimensional constructive interference in steady state to show smaller structures within the CS, making it the ideal choice to study cranial neuropathies in the CS.44
Alterations in signal intensity, size, and contour of the CS are subtle signs of thrombosis. A filling defect with enhancement of the peripheral margins of the CS suggests a clot within it (Fig. 4). Subacute thrombus exhibits high signal intensity on all pulse sequences, whereas acute thrombosis may appear more isointense. Indirect signs that may suggest the diagnosis are dilation of the superior ophthalmic veins, exophthalmos, and increased dural enhancement along the lateral border of CS and ipsilateral tentorium. Appropriate clinical symptoms, adjacent sinusitis, and orbital or odontogenic infection confirm the diagnosis and etiology.33,38,41,43
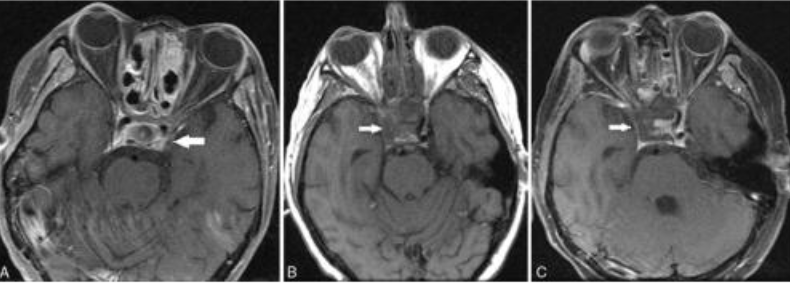
FIGURE 4. (A) Twenty-year-old man with invasive fungal sinusitis in setting of relapsed acute lymphocytic leukemia. Axial postcontrast image of the orbit and CS demonstrates filling defect in the left CS (arrow).
(B and C) Twenty-three-year old man with leukemia and rapidly progressive right-sided cranial neuropathy involving III, IV, and VI. Axial pre- (B) and post (C) contrast T1 images shows filling defect in the right CS with absence of the right cavernous carotid artery flow void (arrows).
CST therapy relies on mobilization of the varied disciplines of neurology, neurosurgery, otolaryngology, and infectious disease. Aggressive antibiotic therapy and surgical debridement of the primary site of infection and surrounding areas of involvement are the mainstay of treatment. The use of steroid therapy to reduce orbital edema and cranial nerve inflammation is controversial. Anticoagulant therapy has shown some benefit when initiated early.33,38,43