Questions:
1. What are 10 causes of ptosis at birth?
2. What are the 4 categories of acquired unilateral or bilateral ptosis?
3. What are 5 types of acquired mechanical ptosis?
4. What are 4 conditions that cause acquired myogenic ptosis?
5. What are 2 causes of an acquired disorder of neuromuscular transmission?
6. What are 3 conditions that cause acquired neurogenic ptosis?
7. Is aponeurotic ptosis usually unilateral or bilateral?
8. What upper eyelid exam findings are likely to be present with aponeurotic ptosis?
9. What is the most common condition causing acquired ptosis in patients over age 50?
10. What usually causes acquired ptosis in young patients?
11. In addition to measuring eyelid positions and levator function, what 2 exam techniques should be performed in all patients with ptosis?
12. What condition must be ruled out in all patients with presumed myogenic ptosis?
13. In Horner syndrome, what is the cause of ptosis?
14. What happens to the ptosis from Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
15. What happens to the pupils in Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
____________________________________________________
Questions with answers:
1. What are 10 causes of ptosis at birth?
1. Congenital ptosis
2. Marcus Gunn jaw winking
3. Trigemino-oculomotor synkinesis
4. Congenital fibrosis
5. Blepharophimosis syndrome
6. Congenital (neonatal) myasthenia
7. Congenital third nerve palsy
8. Birth trauma
9. Lid tumors
10. Orbital tumors
2. What are the 4 categories of acquired unilateral or bilateral ptosis?
1. Mechanical ptosis
2. Myogenic ptosis
3. Disorder of neuromuscular transmission
4. Neurogenic ptosis
3. What are 5 types of acquired mechanical ptosis?
1. Aponeurotic defect
2. Dermatochalasis
3. Cicatricial
4. Tumor (eyelid or orbit)
5. Inflammation (edema, allergy, chalazion, blepharitis, blepharochalasis)
4. What are 4 conditions that cause acquired myogenic ptosis?
1. Chronic progressive external ophthalmoplegia (CPEO)
2. Myotonic dystrophy
3. Oculopharyngeal dystrophy
4. Chronic use of topical ocular steroid drops
5. What are 2 causes of an acquired disorder of neuromuscular transmission?
1. Myasthenia gravis
2. Botulism
6. What are 3 conditions that cause acquired neurogenic ptosis?
1. Horner syndrome (oculosympathetic paresis)
2. Third nerve palsy
3. Apraxia of lid opening
7. Is aponeurotic ptosis usually unilateral or bilateral?
Bilateral
8. What upper eyelid exam findings are likely to be present with aponeurotic ptosis?
The eyelid crease is high or indistinct, and levator function is relatively well preserved.
9. What is the most common condition causing acquired ptosis in patients over age 50?
Aponeurotic ptosis
10. What usually causes acquired ptosis in young patients?
Contact lenses
11. In addition to measuring eyelid positions and levator function, what 2 exam techniques should be performed in all patients with ptosis?
Palpation and eversion of the eyelids
12. What condition must be ruled out in all patients with presumed myogenic ptosis?
Myasthenia gravis
13. In Horner syndrome, what is the cause of ptosis?
Denervation of Müller muscle and inferior tarsal muscle.
14. What happens to the ptosis from Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
It resolves.
15. What happens to the pupils in Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
The anisocoria is reversed.
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
17 Disorders of the Eyelid
The eyelid protects the eye and helps maintain the corneal tear film. Eyelid disorders compromise vision by covering the eye (and covering the visual axis) or by exposing the cornea (resulting in abnormal tear film and blurry vision and complications from corneal exposure).Abnormalities of the eyelid commonly encountered in neuro-ophthalmology include ptosis (drooping of the eyelid), retraction (abnormal elevation of the eyelid), facial weakness (incomplete eyelid closure), and abnormal blinking (decreased or increased).
17.1 Anatomy and Examination of the Eyelid
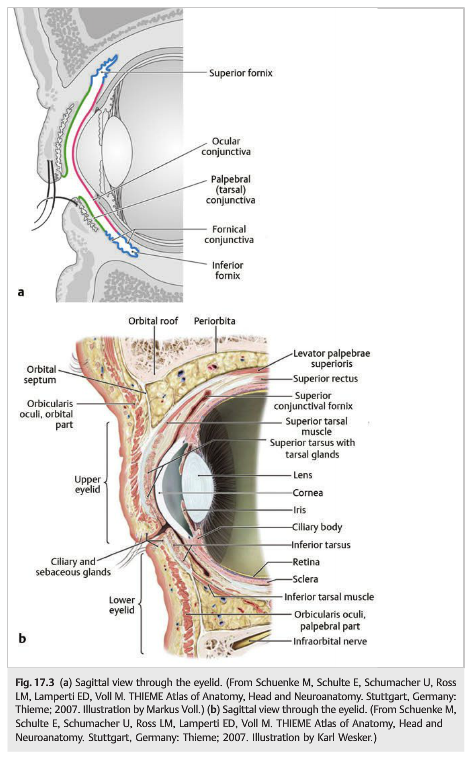
Eyelid closure (▶Fig. 17.2, ▶Fig. 17.3) involves the orbicularis oculi muscle (innervated by branches of the facial nerve: cranial nerve [CN] VII).
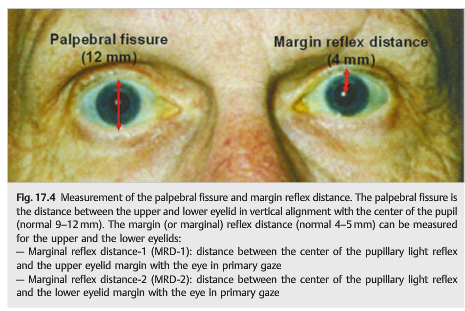
Eyelid opening involves the frontalis muscle (facial nerve), the levator palpebrae (oculomotor nerve: CN III), the Müller muscle and inferior tarsal muscles (sympathetic innervation), and the aponeurosis of the levator muscle attached to the superior tarsal plate. Eyelid position depends on the resting tone of the levator muscle, which varies with the patient’s state of arousal. Eyelid movements are coordinated with vertical eye movements: the eyelids move up and down with the eyes. Examination of the eyelid includes evaluation of the position of the eyelids (looking for possible ptosis and retraction) and lid function, and inspection of the eyelid for any swelling or mass. It includes measurements of the palpebral fissure (9–12mm), the margin reflex distance (4–5 mm), and the levator function, or the difference of position of the lid margin when the patient looks down, then up (>12mm) (▶Fig. 17.4).
Palpation and inversion of the eyelids should be performed in all patients with ptosis. When the eyelids are abnormal, the examiner should look for the presence of an orbital syndrome, diplopia with abnormal extraocular movements, and pupillary abnormalities, and should determine whether the findings are unilateral or bilateral.
17.2 Ptosis
Ptosis can be either congenital or acquired.
17.2.1 Congenital Ptosis
Congenital ptosis is present at birth or early childhood. It can be isolated or accompanied by an elevation deficit of the eye (elevator palsy). There is also incomplete lowering of the eyelid in downgaze, resulting in lid lag. The abnormal eyelid does not stretch well in downgaze (▶Fig. 17.6) because there is congenital maldevelopment of the levator palpebrae or its tendon.
Causes of lid droop at birth include the following:
● Congenital ptosis
● Marcus Gunn jaw winking
● Congenital fibrosis
● Blepharophimosis syndrome (bilateral ptosis, telecanthus, epicanthus inversus)
● Congenital (neonatal) myasthenia
● Congenital third nerve palsy
● Birth trauma (third nerve palsy, Horner syndrome)
● Lid or orbital tumors (neurofibroma, hemangioma, dermoid)
Marcus Gunn jaw winking is a form of congenital ptosis associated with trigemino-oculomotor synkinesis (▶Fig. 17.7)



● Ptotic eyelid that retracts during contraction of the external pterygoid muscle (e.g., while sucking, opening the mouth, or moving the jaw)
● Aberrant connection between the motor branches of the trigeminal nerve (CN V3)innervating the external pterygoid muscle and the fibers of the superior division of the oculomotor nerve (CN III) that innervate the levator superioris muscle of the upper eyelid (trigemino-oculomotor synkinesis)
17.2.2 Acquired Ptosis
Causes of acquired unilateral or bilateral ptosis include the following:
● Mechanical ptosis
○ Aponeurotic defect(▶Fig. 17.8) (levator dehiscence)
– Aging
– Trauma, surgery (ocular with use of speculum, orbital)
– Contact lens use
○ Dermatochalasis
○ Cicatricial
○ Eyelid or orbital tumor
○ Inflammation
– Edema
– Allergy
– Chalazion
– Blepharitis
– Blepharochalasis
● Myogenic ptosis
○ Chronic progressive external ophthalmoplegia (CPEO)
○ Myotonic dystrophy
○ Oculopharyngeal dystrophy
○ Chronic use of topical ocular steroid drops
● Disorder of neuromuscular transmission
○ Myasthenia gravis
○ Botulism
● Neurogenic ptosis
○ Horner syndrome (oculosympathetic paresis)
○ Third nerve palsy
○ Apraxia of lid opening
Mechanical Ptosis
Aponeurotic ptosis (▶Fig. 17.8) is usually bilateral. The upper eyelid crease is high or indistinct, and levator function is relatively preserved.

In elderly patients, an aponeurotic defect may be associated with dermatochalasis. The aponeurosis of the levator muscle dehisces or disinserted from the tarsal plate of the upper lid (usually bilateral). It is also common after ocular surgery requiring a speculum (usually unilateral). In younger patients, it is usually secondary to contact lens wear.
Pearls
Aponeurotic defect is the most common cause of acquired ptosis in adults.
Lesions of the eyelid (e.g., tumor, chalazion, and vascular malformations) can produce a mechanical ptosis (▶Fig. 17.9 and Fig. 17.10).
Pearls
Palpation and inversion of the eyelids should be performed in all patients with ptosis.
Myogenic Ptosis
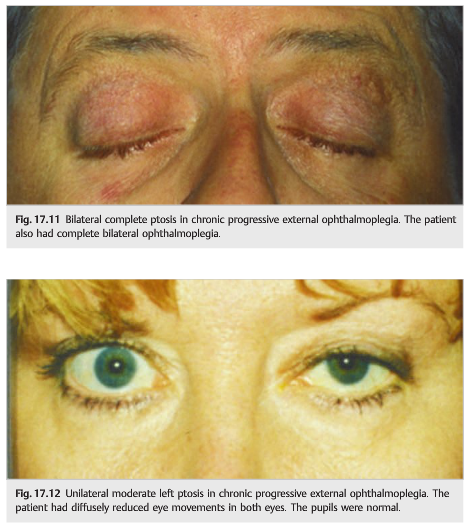
Myogenic ptosis (▶Fig. 17.11 and Fig. 17.12) is usually bilateral and progressive. It is commonly associated with impaired eye movements. There may not be diplopia if the eyes are straight in primary position and if the ophthalmoplegia is complete. The pupils are always normal. Chronic progressive external ophthalmoplegia (mitochondrial disorder) is a classic cause.
Ptosis Resulting from a Neuromuscular Transmission Disorder
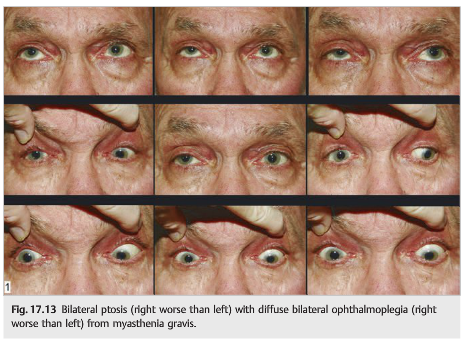
Myasthenia gravis is a classic cause of unilateral or bilateral ptosis (▶Fig. 17.13).Myasthenic ptosis may be isolated, or it may be associated with oculomotor paresis. The pupils are always normal. The hallmark of myasthenic ptosis is fluctuation. The Ptosis usually reverses with a Tensilon test (see Chapter 13).
Neurogenic Ptosis
Lesions of the Oculosympathetic Pathways
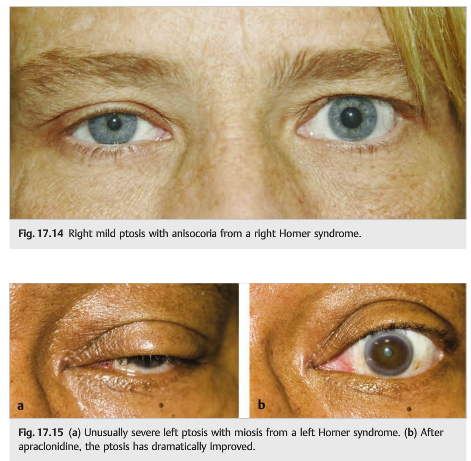
Lesions of the oculosympathetic pathways produce an ipsilateral Horner syndrome, which consists of mild ptosis (reduced palpebral fissure) and impaired dilation of the pupil, with anisocoria worse in the dark and dilation lag (▶Fig. 17.14 and ▶Fig. 17.15a).The ptosis results from denervation of the Müller muscle and inferior tarsal muscle of the lower lid. It is usually mild and usually 1 to 2mm, although 3 or 4mm of ptosis can sometimes be observed. The ptosis from Horner syndrome resolves after administration of topical apraclonidine 0.5% or 1.0%. Apraclonidine drops are useful for the diagnosis of Horner syndrome (it reverses the anisocoria). It can also be used to improve the ptosis (▶Fig. 17.15b).
Lesions of the Third Nerve
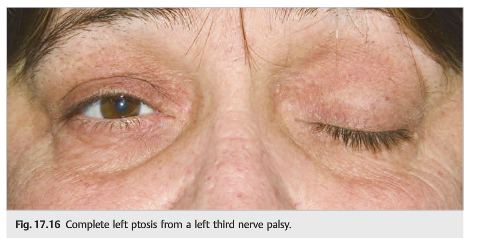
Lesions of the third cranial nerve produce an ipsilateral ptosis. The ptosis results from weakness of the levator palpebrae muscle and may be complete or mild. It is never isolated: the eye movements are abnormal, and the pupil may be dilated. When the ptosis is complete, diplopia may not be noticed by the patient (▶Fig. 17.16). A lesion of the third nerve nucleus in the midbrain produces bilateral ptosis.

Questions:
1. What are 10 causes of ptosis at birth?
2. What are the 4 categories of acquired unilateral or bilateral ptosis?
3. What are 5 types of acquired mechanical ptosis?
4. What are 4 conditions that cause acquired myogenic ptosis?
5. What are 2 causes of an acquired disorder of neuromuscular transmission?
6. What are 3 conditions that cause acquired neurogenic ptosis?
7. Is aponeurotic ptosis usually unilateral or bilateral?
8. What upper eyelid exam findings are likely to be present with aponeurotic ptosis?
9. What is the most common condition causing acquired ptosis in patients over age 50?
10. What usually causes acquired ptosis in young patients?
11. In addition to measuring eyelid positions and levator function, what 2 exam techniques should be performed in all patients with ptosis?
12. What condition must be ruled out in all patients with presumed myogenic ptosis?
13. In Horner syndrome, what is the cause of ptosis?
14. What happens to the ptosis from Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
15. What happens to the pupils in Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
____________________________________________________
Questions with answers:
1. What are 10 causes of ptosis at birth?
1. Congenital ptosis
2. Marcus Gunn jaw winking
3. Trigemino-oculomotor synkinesis
4. Congenital fibrosis
5. Blepharophimosis syndrome
6. Congenital (neonatal) myasthenia
7. Congenital third nerve palsy
8. Birth trauma
9. Lid tumors
10. Orbital tumors
2. What are the 4 categories of acquired unilateral or bilateral ptosis?
1. Mechanical ptosis
2. Myogenic ptosis
3. Disorder of neuromuscular transmission
4. Neurogenic ptosis
3. What are 5 types of acquired mechanical ptosis?
1. Aponeurotic defect
2. Dermatochalasis
3. Cicatricial
4. Tumor (eyelid or orbit)
5. Inflammation (edema, allergy, chalazion, blepharitis, blepharochalasis)
4. What are 4 conditions that cause acquired myogenic ptosis?
1. Chronic progressive external ophthalmoplegia (CPEO)
2. Myotonic dystrophy
3. Oculopharyngeal dystrophy
4. Chronic use of topical ocular steroid drops
5. What are 2 causes of an acquired disorder of neuromuscular transmission?
1. Myasthenia gravis
2. Botulism
6. What are 3 conditions that cause acquired neurogenic ptosis?
1. Horner syndrome (oculosympathetic paresis)
2. Third nerve palsy
3. Apraxia of lid opening
7. Is aponeurotic ptosis usually unilateral or bilateral?
Bilateral
8. What upper eyelid exam findings are likely to be present with aponeurotic ptosis?
The eyelid crease is high or indistinct, and levator function is relatively well preserved.
9. What is the most common condition causing acquired ptosis in patients over age 50?
Aponeurotic ptosis
10. What usually causes acquired ptosis in young patients?
Contact lenses
11. In addition to measuring eyelid positions and levator function, what 2 exam techniques should be performed in all patients with ptosis?
Palpation and eversion of the eyelids
12. What condition must be ruled out in all patients with presumed myogenic ptosis?
Myasthenia gravis
13. In Horner syndrome, what is the cause of ptosis?
Denervation of Müller muscle and inferior tarsal muscle.
14. What happens to the ptosis from Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
It resolves.
15. What happens to the pupils in Horner syndrome after administration of topical apraclonidine 0.5% or 1.0%?
The anisocoria is reversed.
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
17 Disorders of the Eyelid
The eyelid protects the eye and helps maintain the corneal tear film. Eyelid disorders compromise vision by covering the eye (and covering the visual axis) or by exposing the cornea (resulting in abnormal tear film and blurry vision and complications from corneal exposure).Abnormalities of the eyelid commonly encountered in neuro-ophthalmology include ptosis (drooping of the eyelid), retraction (abnormal elevation of the eyelid), facial weakness (incomplete eyelid closure), and abnormal blinking (decreased or increased).
17.1 Anatomy and Examination of the Eyelid
Eyelid closure (▶Fig. 17.2, ▶Fig. 17.3) involves the orbicularis oculi muscle (innervated by branches of the facial nerve: cranial nerve [CN] VII).
Eyelid opening involves the frontalis muscle (facial nerve), the levator palpebrae (oculomotor nerve: CN III), the Müller muscle and inferior tarsal muscles (sympathetic innervation), and the aponeurosis of the levator muscle attached to the superior tarsal plate. Eyelid position depends on the resting tone of the levator muscle, which varies with the patient’s state of arousal. Eyelid movements are coordinated with vertical eye movements: the eyelids move up and down with the eyes. Examination of the eyelid includes evaluation of the position of the eyelids (looking for possible ptosis and retraction) and lid function, and inspection of the eyelid for any swelling or mass. It includes measurements of the palpebral fissure (9–12mm), the margin reflex distance (4–5 mm), and the levator function, or the difference of position of the lid margin when the patient looks down, then up (>12mm) (▶Fig. 17.4).
Palpation and inversion of the eyelids should be performed in all patients with ptosis. When the eyelids are abnormal, the examiner should look for the presence of an orbital syndrome, diplopia with abnormal extraocular movements, and pupillary abnormalities, and should determine whether the findings are unilateral or bilateral.
17.2 Ptosis
Ptosis can be either congenital or acquired.
17.2.1 Congenital Ptosis
Congenital ptosis is present at birth or early childhood. It can be isolated or accompanied by an elevation deficit of the eye (elevator palsy). There is also incomplete lowering of the eyelid in downgaze, resulting in lid lag. The abnormal eyelid does not stretch well in downgaze (▶Fig. 17.6) because there is congenital maldevelopment of the levator palpebrae or its tendon.
Causes of lid droop at birth include the following:
● Congenital ptosis
● Marcus Gunn jaw winking
● Congenital fibrosis
● Blepharophimosis syndrome (bilateral ptosis, telecanthus, epicanthus inversus)
● Congenital (neonatal) myasthenia
● Congenital third nerve palsy
● Birth trauma (third nerve palsy, Horner syndrome)
● Lid or orbital tumors (neurofibroma, hemangioma, dermoid)
Marcus Gunn jaw winking is a form of congenital ptosis associated with trigemino-oculomotor synkinesis (▶Fig. 17.7)
● Ptotic eyelid that retracts during contraction of the external pterygoid muscle (e.g., while sucking, opening the mouth, or moving the jaw)
● Aberrant connection between the motor branches of the trigeminal nerve (CN V3)innervating the external pterygoid muscle and the fibers of the superior division of the oculomotor nerve (CN III) that innervate the levator superioris muscle of the upper eyelid (trigemino-oculomotor synkinesis)
17.2.2 Acquired Ptosis
Causes of acquired unilateral or bilateral ptosis include the following:
● Mechanical ptosis
○ Aponeurotic defect(▶Fig. 17.8) (levator dehiscence)
– Aging
– Trauma, surgery (ocular with use of speculum, orbital)
– Contact lens use
○ Dermatochalasis
○ Cicatricial
○ Eyelid or orbital tumor
○ Inflammation
– Edema
– Allergy
– Chalazion
– Blepharitis
– Blepharochalasis
● Myogenic ptosis
○ Chronic progressive external ophthalmoplegia (CPEO)
○ Myotonic dystrophy
○ Oculopharyngeal dystrophy
○ Chronic use of topical ocular steroid drops
● Disorder of neuromuscular transmission
○ Myasthenia gravis
○ Botulism
● Neurogenic ptosis
○ Horner syndrome (oculosympathetic paresis)
○ Third nerve palsy
○ Apraxia of lid opening
Mechanical Ptosis
Aponeurotic ptosis (▶Fig. 17.8) is usually bilateral. The upper eyelid crease is high or indistinct, and levator function is relatively preserved.
In elderly patients, an aponeurotic defect may be associated with dermatochalasis. The aponeurosis of the levator muscle dehisces or disinserted from the tarsal plate of the upper lid (usually bilateral). It is also common after ocular surgery requiring a speculum (usually unilateral). In younger patients, it is usually secondary to contact lens wear.
Pearls
Aponeurotic defect is the most common cause of acquired ptosis in adults.
Lesions of the eyelid (e.g., tumor, chalazion, and vascular malformations) can produce a mechanical ptosis (▶Fig. 17.9 and Fig. 17.10).
Pearls
Palpation and inversion of the eyelids should be performed in all patients with ptosis.
Myogenic Ptosis
Myogenic ptosis (▶Fig. 17.11 and Fig. 17.12) is usually bilateral and progressive. It is commonly associated with impaired eye movements. There may not be diplopia if the eyes are straight in primary position and if the ophthalmoplegia is complete. The pupils are always normal. Chronic progressive external ophthalmoplegia (mitochondrial disorder) is a classic cause.
Ptosis Resulting from a Neuromuscular Transmission Disorder
Myasthenia gravis is a classic cause of unilateral or bilateral ptosis (▶Fig. 17.13).Myasthenic ptosis may be isolated, or it may be associated with oculomotor paresis. The pupils are always normal. The hallmark of myasthenic ptosis is fluctuation. The Ptosis usually reverses with a Tensilon test (see Chapter 13).
Neurogenic Ptosis
Lesions of the Oculosympathetic Pathways
Lesions of the oculosympathetic pathways produce an ipsilateral Horner syndrome, which consists of mild ptosis (reduced palpebral fissure) and impaired dilation of the pupil, with anisocoria worse in the dark and dilation lag (▶Fig. 17.14 and ▶Fig. 17.15a).The ptosis results from denervation of the Müller muscle and inferior tarsal muscle of the lower lid. It is usually mild and usually 1 to 2mm, although 3 or 4mm of ptosis can sometimes be observed. The ptosis from Horner syndrome resolves after administration of topical apraclonidine 0.5% or 1.0%. Apraclonidine drops are useful for the diagnosis of Horner syndrome (it reverses the anisocoria). It can also be used to improve the ptosis (▶Fig. 17.15b).
Lesions of the Third Nerve
Lesions of the third cranial nerve produce an ipsilateral ptosis. The ptosis results from weakness of the levator palpebrae muscle and may be complete or mild. It is never isolated: the eye movements are abnormal, and the pupil may be dilated. When the ptosis is complete, diplopia may not be noticed by the patient (▶Fig. 17.16). A lesion of the third nerve nucleus in the midbrain produces bilateral ptosis.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.