Questions:
34. A patient has infectious meningitis with severe papilledema. What risk does this pose and what treatment is appropriate?
35. A patient presents with slowly progressive memory loss, cognitive impairment, oculomasticatory movements (myorhythmia), supranuclear vertical gaze palsy. What curable condition should be considered and what lab tests can be used to make the diagnosis?
36. What are 3 classic causes of raised ICP in a patient with known cancer? 37. What are the neuro-ophthalmic manifestations of paraneoplastic syndromes?
_________________________________________
Questions with answers:
34. A patient has infectious meningitis with severe papilledema. What risk does this pose and what treatment is appropriate?
Infectious meningitis often produces an increase in intracranial pressure and severe papilledema. Visual loss from unrecognized papilledema is a common cause of nonreversible visual loss in meningitis. Repeat lumbar punctures and treatment of intracranial hypertension are crucial in this setting. Acute bacterial meningitis, tuberculous meningitis, and cryptococcal meningitis are particularly frequently associated with severe papilledema and visual loss.
35. A patient presents with slowly progressive memory loss, cognitive impairment, oculomasticatory movements (myorhythmia), supranuclear vertical gaze palsy. What curable condition should be considered and what lab tests can be used to make the diagnosis?
Whipple Disease: This rare disorder is often discussed in neuro-ophthalmology because it is frequently associated with eye movement abnormalities. It is caused by a gram-positive bacillus (Tropheryma whipplei), which mostly resides in the gut.
Diagnostic tests:
1. Positive polymerase chain reaction (PCR) for Tropheryma whipplei in the cerebrospinal fluid
2. Positive polymerase chain reaction (PCR) for Tropheryma whipplei in the jejunal biopsy.
3. Biopsy of jejunal mucosa periodic acid-Schiff stain
Treatment consists of long-term antibiotics.
36. What are 3 classic causes of raised ICP in a patient with known cancer?
1. metastasis
2. carcinomatous meningitis
3. cerebral venous thrombosis (often from cancer-induced hypercoagulable state)
37. What are the neuro-ophthalmic manifestations of paraneoplastic syndromes?
1. Abnormal eye movements – Opsoclonus (Ri antibodies), Ocular flutter (Ri antibodies), Cerebellar degeneration (Yo antibodies), Nystagmus, Slow saccades/limited vertical movements (Hu, Ma/Ta antibodies)
2. Neuromuscular junction disorders – Lambert Eaton or myasthenia ( Voltage-gated calcium channel antibodies)
3. Visual loss: Cancer-associated retinopathy (CAR antibodies), Melanoma-associated retinopathy (MAR antibodies), Optic neuropathy with disc edema and intraocular inflammation (CRMP-5 antibodies)
_________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
20.6 Infectious Diseases
Systemic infections can produce various neuro-ophthalmic manifestations. Infections can invade the intracranial space, the orbit, and the eye and can produce visual loss, visual field defects, and diplopia.
All infections (bacterial, viral, fungal, and parasitic) may invade the central nervous system and the eye, although some have a particular tropism for these organs. For example, cryptococcal infection (fungus) is a classic cause of acute meningitis in immunodeficient patients; secondary and tertiary syphilis (spirochete) are classic causes of meningitis, uveitis, and optic neuritis; zoster virus infection produces ocular signs and often ophthalmoplegia when involving the first branch of the trigeminal nerve; cat scratch disease (Bartonella henselae infection) is a classic cause of neuroretinitis.
The neurologic and ocular complications of systemic infections include the following:
● Intracranial infection
○ Cerebral abscess
○ Cerebral empyema
○ Infectious meningitis
○ Optic neuritis
○ Encephalitis
○ Ventriculitis
○ Vasculitis
– Cerebral infarction
– Cerebral hemorrhages
○ Cavernous sinus abscess or thrombosis
● Orbital cellulitis
● Ocular infection
○ Endophthalmitis
○ Retinitis
○ Choroiditis
● Endocarditis
○ Cerebral infarction
○ Mycotic intracranial aneurysm
○ Retinal emboli (Roth spots)
● Cerebral venous thrombosis
○ Raised intracranial pressure (papilledema)
○ Venous infarction
Pearls
Infectious meningitis often produces an increase in intracranial pressure and severe papilledema. Visual loss from unrecognized papilledema is a common cause of non-reversible visual loss in meningitis. Repeat lumbar punctures and treatment of intracranial hypertension are crucial in this setting. Acute bacterial meningitis, tuberculous meningitis, and cryptococcal meningitis are particularly frequently associated with severe papilledema and visual loss.
20.6.1 Syphilis
Fig.20.42 a,b Bilateral papilledema in a patient with secondary syphilis and chronic lymphocytic meningitis. This patient was found to be positive for HIV.
Neuro-ophthalmic complications of syphilis (▶Fig. 20.42) include the following:
● Uveitis (all types)
● Retinitis
● Choroiditis
● Optic neuritis
● Lymphocytic meningitis
○ Papilledema
○ Basilar meningitis with cranial nerve palsies
○ Vasculitis
– Cerebral infarction
● Intracranial mass (gumma)

20.6.2 Acquired Immunodeficiency Syndrom
Posterior segment manifestations of acquired immunodeficiency syndrome (AIDS)include the following (▶Fig. 20.43,▶Fig. 20.44,▶Fig. 20.45,▶Fig. 20.46):
● Infectious
○ Herpes zoster ophthalmicus and optic neuritis
○ Herpes simplex optic neuritis
○ Progressive outer retinal necrosis (PORN)
○ Cytomegalovirus retinitis and optic neuritis
○ Toxoplasmosis chorioretinitis and optic neuritis
○ Syphilis retinitis and optic neuritis
○ Pneumocystis jiroveci (formerly P. carinii) choroiditis
○ Fungal choroiditis
○ Papilledema from meningitis (cryptococcal meningitis most common)
● Noninfectious
○ Retinal microvasculopathy
○ Retinal cotton wool spots
○ Ocular lymphoma
○ HIV optic neuritis



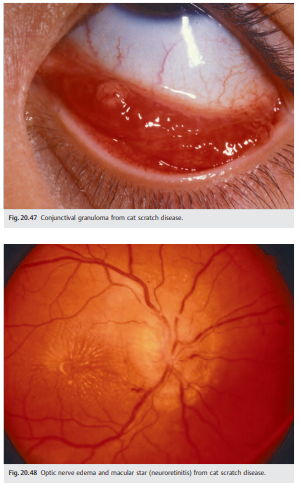
20.6.3 Cat Scratch Disease (Bartonella Henselae Infection)
Bartonella henselae infection produces various ocular manifestations, including anterior segment inflammation, retinitis, and optic neuritis (▶Fig. 20.47 and ▶Fig. 20.48). Retinal vascular occlusions are also common.
20.6.4 Whipple Disease
This rare disorder is often discussed in neuro-ophthalmology because it is frequently associated with eye movement abnormalities. It is caused by a gram-positive bacillus (Tropheryma whipplei), which mostly resides in the gut.
Clinical Presentation
● Weight loss, fever
● Diarrhea, abdominal pain
● Arthralgias
● Lymphadenopathy
● Neurologic manifestations (may be isolated):
○ Slowly progressive memory loss with cognitive impairment
○ Oculomasticatory movements (myorhythmia)
○ Supranuclear vertical (more than horizontal) gaze palsy
Diagnosis
● Positive polymerase chain reaction (PCR) for Tropheryma whipplei in the
CSF
● Biopsy of jejunal mucosa with periodic acid-Schiff stain (PAS-positive organisms)
● Positive PCR for Tropheryma whipplei in the jejunal biopsy
Treatment
Treatment consists of long-term antibiotics.
Tumors
Intracranial tumors (all types) often produce neuro-ophthalmic symptoms and signs.
20.6.5 Mechanisms
The mechanisms by which brain tumors produce neuro-ophthalmic symptoms and signs include the following.
● Raised intracranial pressure (from the mass or from obstructive hydrocephalus)
○ Papilledema
○ Diplopia (from sixth nerve palsy)
● Mass effect or infiltration
○ Choroidal metastasis
○ Intracranial optic nerve (optic neuropathy)
○ Chiasm (bitemporal hemianopia)
○ Retrochiasmal visual pathways (homonymous hemianopia)
○ Ocular motor cranial nerve (diplopia)
● Carcinomatous meningitis
○ Raised intracranial pressure
○ Multiple cranial nerve palsies
● Paraneoplastic syndrome from a cancer
○ Retinopathy
○ Optic neuropathy
○ Nystagmus, opsoclonus, brainstem syndromes
● Toxicity of treatment
○ Postsurgical complication
○ Radiation
– Radiation necrosis of the brain
– Radiation optic neuropathy (see Chapter 8)
– Radiation retinopathy
○ Chemotherapy
– Optic nerve toxicity
Cancer patients who develop neuro-ophthalmic symptoms or signs (such as optic neuropathy, papilledema, visual field defect, diplopia, or nystagmus) need immediate neuroimaging (MRI of the brain, often with the orbits, and with contrast). If the imaging is normal, then a lumbar puncture with CSF opening pressure, cytology, and flow cytometry needs to be performed.
20.6.6 Carcinomatous Meningitis
Carcinomatous meningitis must be ruled out in all patients with raised intracranial pressure and a known history of cancer. Imaging is often normal or may show leptomeningeal enhancement. A lumbar puncture with CSF opening pressure and CSF analysis, including cytology and flow cytometry, is mandatory. If normal, the lumbar puncture should be repeated for repeat cytologic examination. Sometimes, it is necessary to perform at least three lumbar punctures to make a diagnosis of carcinomatous meningitis.
The most common sites or types of cancer in patients with carcinomatous meningitis are as follows:
● Breast
● Lung
● Lymphoma
● Melanoma
● Adenocarcinoma of unknown origin
Pearls
The three classic causes of raised intracranial pressure in patients with known cancer are (1) metastasis, (2) carcinomatous meningitis, (3) cerebral venous thrombosis (from cancer-induced hypercoagulable state).
20.6.7 Paraneoplastic Syndromes
Paraneoplastic syndromes represent rare nonmetastatic complications of cancer, which can affect multiple levels of the nervous system. Autoantibodies are usually found in the CSF or serum. Paraneoplastic syndromes may complicate a known cancer or may be the first sign of a very localized cancer.
Neuro-ophthalmic symptoms and signs are relatively common and include the following:
● Abnormal eye movements
○ Opsoclonus (Ri antibodies)
○ Ocular flutter (Ri antibodies)
○ Cerebellar degeneration (Yo antibodies)
○ Nystagmus
○ Slow saccades, limited vertical movements (Hu, Ma/Ta antibodies)
● Neuromuscular junction disorder (Lambert–Eaton syndrome or myasthenic syndrome)
○ Voltage-gated calcium channel antibodies
● Visual loss
○ Retinal degeneration
– Cancer-associated retinopathy (CAR) antibodies
– Melanoma-associated retinopathy (MAR) antibodies
○ Optic neuropathy with disc edema and intraocular inflammation
– CRMP-5 antibodies
20.7 Traumatic Brain Injury
Neuro-ophthalmic manifestations of traumatic brain injury include the following:
● Visual loss
○ Monocular
– Trauma to the eye
– Orbital trauma
– Optic nerve injury (direct/indirect)
○ Binocular
– Trauma to both eyes or both optic nerves
– Traumatic chiasmopathy (bitemporal hemianopia)
– Trauma to the retrochiasmal visual pathways (homonymous hemianopia)
○ Higher cortical function impairment from brain injury
● Diplopia
○ Orbital trauma (entrapment, fibrosis of extraocular muscles)
○ Cranial nerve palsies (fourth, sixth, and third)
○ Intracranial lesions
Causes of post-traumatic acute visual loss include the following:
● Refractive error
○ Glasses or contact lenses are lost or damaged at the time of trauma (may
be overlooked in patients with difficulty communicating)
● Ocular injury
○ Ruptured globe (anterior with corneal laceration or posterior with scleral laceration)
○ Intraocular foreign body
○ Exposure keratopathy (secondary to proptosis, lid laceration, or seventh nerve dysfunction)
○ Corneal edema (from airbag injury)
○ Corneal abrasion
○ Hyphema (blood in anterior chamber)
○ Traumatic iritis (often delayed by about 24 hours)
○ Traumatic mydriasis (and decreased accommodation)
○ Lens subluxation or luxation
○ Vitreous hemorrhage
○ Commotio retinae
○ Retinal detachment
○ Retinal ischemia from carotid dissection
○ Retinal fat emboli
○ Choroidal rupture
● Optic nerve
○ Direct traumatic optic neuropathy
○ Indirect traumatic optic neuropathy
○ Intrasheath hematoma
○ Avulsion of the optic nerve head
○ Penetrating injuries of the orbit with direct optic nerve injury
○ Intraorbital foreign body
○ Optic nerve ischemia from carotid dissection
● Orbit
○ Orbital fracture (direct optic nerve damage)
○ Orbital hemorrhage (optic nerve ischemia)○ Orbital emphysema (optic nerve ischemia)
○ Carotid cavernous fistula (increased intraocular pressure)
○ Subperiosteal hemorrhage (direct optic nerve damage or optic nerve ischemia)
● Intracranial optic pathways
○ Chiasmal or retrochiasmal direct injury
○ Chiasmal or retrochiasmal indirect injury
○ Hemorrhage or hematoma compressing the chiasm
○ Cerebral diffuse axonal injury with homonymous hemianopia
○ Intraparenchymal hemorrhage with homonymous hemianopia
○ Cerebral infarction (posterior cerebral artery) secondary to increased intracranial pressure/herniation with homonymous hemianopia or cerebral blindness
○ Cerebral infarction secondary to cervical artery dissection with homonymous hemianopia
20.8 Visual Loss during Ocular or Cranial Surgery
Damage to the intracranial visual pathways or to the optic nerves may occur during surgery. Visual loss is particularly common during ocular and intracranial surgery, but it may occur as a complication of any surgical procedure. The first step when evaluating a patient with postoperative visual loss is to localize the lesion by an ophthalmic examination.
Visual loss during ocular surgery can result from the following:
● Optic neuropathy
○ Direct damage to the retrobulbar optic nerve from retrobulbar anesthesia, orbital surgery, orbital hemorrhage after blepharoplasty
○ Fluctuation in intraocular pressure during ocular surgery
○ Postoperative intraocular hypertension
● Diplopia
○ Direct damage to the extraocular muscles from the following:
– Retrobulbar anesthesia
– Orbital surgery
– Orbital hemorrhage after blepharoplasty
– Scleral buckle placed for treatment of a retinal detachment
● Ptosis
○ Damage of the levator muscle from the ocular speculum
Visual loss during cranial surgery can result from compression, edema, ischemia, hemorrhage, or direct injury to the intracranial optic nerve, the chiasm, or the intracranial retrochiasmal visual pathways.
Visual loss during nonocular, noncranial surgery can result from the following:
● Anterior segment lesion
○ Corneal abrasion
○ Trauma (pressure on the eye during surgery)
○ Reversible retinal toxicity after prostate surgery (irrigating solution)
● Ocular ischemia
○ Central retinal artery occlusion
○ Ischemic optic neuropathy (anterior and posterior)
● Chiasmal lesion
○ Pituitary apoplexy
● Intracranial ischemia (homonymous hemianopia or cerebral blindness)
Ischemic optic neuropathies are particularly common after coronary artery bypass graft and after spinal surgery. Their mechanism remains debated.
Retinal and optic nerve ischemia may also occur during any procedure complicated by major bleeding with severe hypotension and after procedures involving the cervical vessels or dissection of the neck.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.ed
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu .