Questions:
16. What condition should be considered in any patient over 50 with transient or constant diplopia?
17. What condition should be considered in any patient over 50 with headaches
18. Is Cranial Arteritis common, uncommon, or rare among Blacks, Hispanics, Asians, and Whites?
19. What percent of patients will have premonitory visual symptoms, usually within the week preceding permanent visual loss from Cranial Arteritis?
20. What are the 7 ophthalmic signs in a patient with anterior ischemic optic neuropathy that are highly suggestive of Cranial Arteritis?
21. In what percentage of patients with Cranial Arteritis will the ESR be normal?
22. Is the CRP ever normal in Cranial Arteritis?
23. What other blood tests may be elevated in Cranial Arteritis?
24. How long will patients with Cranial Arteritis generally need to be treated with oral steroids?
25. At what rate should oral prednisone be tapered in Cranial Arteritis?
26. What test is the only test that confirms the diagnosis of temporal arteritis?
_________________________________________________
Questions with answers:
16. What condition should be considered in any patient over 50 with transient or constant diplopia?
Cranial arteritis
17. What condition should be considered in any patient over 50 with headaches?
Cranial arteritis
18. Is Cranial Arteritis common, uncommon, or rare among Blacks, Hispanics, Asians, and Whites?
It is more prevalent in whites, relatively uncommon in blacks, and is rare in Hispanics and Asians.
19. What percent of patients will have visual symptoms the week preceding permanent visual loss from Cranial Arteritis?
65%
20. What are the 7 ophthalmic signs in a patient with anterior ischemic optic neuropathy that are highly suggestive of Cranial Arteritis?
1. A large cup-to-disc ratio (no “disc-at-risk” for nonarteritic AION)
2. Pale/milky/chalky white optic disc edema acutely
3. Cotton wool spots suggesting associated retinal ischemia
4. Choroidal ischemia
5. Transient visual loss preceding the AION
6. Transient diplopia preceding the AION
7. Orbital or ocular pain
21. In what percentage of patients with Cranial Arteritis will the ESR be normal?
20%
22. Is the CRP ever normal in Cranial Arteritis?
Yes, but this is extremely rare.
23. What other blood tests may be elevated in Cranial Arteritis?
Platelets and fibrinogen are often elevated, and the hematocrit is often low.
24. How long will patients with Cranial Arteritis generally need to be treated with oral steroids?
Usually, they will need to be treated for 1 to 2 years and sometimes longer.
25. At what rate should oral prednisone be tapered in Cranial Arteritis?
As a general rule, the taper should be slow in the range of 10 mg/month reaching 20 mg/day at 6 months and 10 mg/day at 1 year. Patients are seen monthly while tapering the prednisone for neuro-ophthalmic examination, evaluation of side effects, and biological markers. Any clinical or biological indication of activity of the disease should result in an increase of the steroids and a slower taper.
26. What test is the only test that confirms the diagnosis of temporal arteritis?
Temporal artery biopsy is the only definite confirmation of the diagnosis. It must always be performed, as long term steroids have potentially serious side effects. A false-negative biopsy occurs in about 4 to 5% of cases.
_________________________________________________
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
20.3 Giant Cell Arteritis
Giant cell arteritis (temporal arteritis, cranial arteritis, or Horton disease) is an inflammatory vasculopathy of the medium and large arteries, with a propensity to affect the aorta and its extracranial branches. It is the most common primary vasculitis in adults, occurring almost exclusively in individuals older than 50 years and being much more common in patients older than 70. It is more prevalent in whites, relatively uncommon in blacks, and rare in Hispanics.
20.3.1 Patient Evaluation
Patients with giant cell arteritis present clinically as follows:
● Systemic symptoms (polymyalgia rheumatic)
● Ocular symptoms with permanent, devastating visual loss(usually follow the systemic symptoms, but can be isolated in 25%of cases)
Pearls
○ The diagnosis of giant cell arteritis must be made prior to visual loss. Immediate Treatment with steroids prevents visual loss.
○ Headaches or visual loss in a patient older than 50 should raise the possibility of giant cell arteritis.
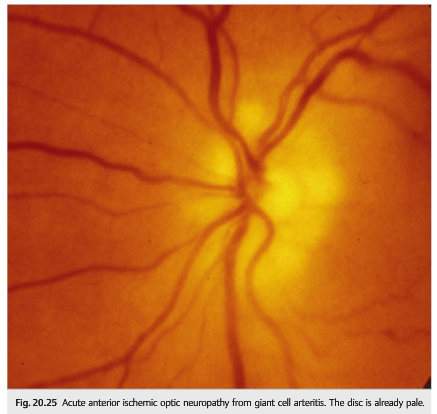
○ Anterior ischemic optic neuropathy (AION) is the most common ophthalmic manifestation of giant cell arteritis (▶Fig. 20.25 and ▶Fig. 20.26).

Posterior Ischemic optic neuropathy (PION) may also occur in giant cell arteritis, but caution is advised when making this diagnosis because ophthalmic artery aneurysms, pituitary apoplexy, and tumor infiltration are also classic causes of acute or subacute retrobulbar optic neuropathy in this age group.
○ Always consider giant cell arteritis in the differential diagnosis of older patients with diplopia. The diplopia associated with giant cell arteritis may be transient, particularly when the cause is extraocular muscle ischemia.
Non-neuro-ophthalmic Manifestations of Giant Cell Arteritis
Systemic symptoms are very common and include the following:
● Headache (most common)
● Temporal artery abnormalities (prominence, tenderness, pulselessness)
● Systemic symptoms and signs of vasculitis (polymyalgia rheumatica):
○ Fever
○ Asthenia
○ Arthralgias, peripheral synovitis
○ Myalgias
○ Weight loss/Anorexia
○ Cough
● Ischemic complications
○ Jaw claudication
○ Scalp necrosis
○ Tongue necrosis
○ Sore throat
○ Hoarseness
○ Cerebral infarction or transient ischemic attack
○ Angina, myocardial infarction
○ Upper extremity ischemia (pain, claudication)
● Mental status changes
○ Depression
○ Delusions
○ Memory impairment/dementia
Neuro-ophthalmic Manifestations of Giant Cell Arteritis
25% of patients with giant cell arteritis develop visual symptoms without systemic symptoms. They include the following:
● Permanent visual loss occurs in 15 to 20% of patients with giant cell arteritis.
● Visual loss associated with giant cell arteritis usually results from one or more of the following:
○ Optic nerve ischemia (vasculitic involvement of the short posterior ciliary arteries)
○ Choroidal ischemia (also vascularized by posterior ciliary arteries)
○ Retinal infarction (less common; vasculitic involvement of the central retinal artery)
○ Bilateral occipital infarction (exceedingly rare in giant cell arteritis)
● Diplopia occurs in up to 15% of patients with giant cell arteritis.
○ Results most often from ischemia of the extraocular muscles (orbital ischemia), although cranial nerve involvement or brainstem ischemia may also occur in giant cell arteritis
Pearls
Visual loss in arteritic ischemic optic neuropathy is usually severe (hand motion to no light perception vision) and usually permanent. It may be preceded by recurrent episodes of transient monocular visual loss or transient diplopia (premonitory visual symptoms occur in about 65% of patients, usually within the week preceding permanent visual loss)
Summary of the Neuro-ophthalmic Manifestations of Giant Cell Arteritis
● Optic neuropathy
○ Anterior ischemic optic neuropathy
○ Posterior ischemic optic neuropathy
● Retinal ischemia○ Central retinal artery occlusion
○ Branch retinal artery occlusion
○ Diffuse or focal retinal ischemic
○ Cotton Wool spots
○ Retinal hemorrhages
● Choroidal ischemia
● Ocular ischemic syndrome
○ Corneal edema
○ Anterior uveitis
○ Cataract
○ Increased intraocular pressure (neovascular glaucoma)
○ Ocular hypotony
○ Retinal hemorrhages (venous stasis retinopathy)
○ Retinal neovascularization
● Orbital ischemia
○ Orbital pain
○ Diplopia (ischemia of the extraocular muscles)
○ Proptosis
● Cranial nerve ischemia
○ Diplopia (third, fourth, and sixth nerve ischemia)
● Cerebral ischemia
○ Brainstem ischemia (diplopia)
○ Occipital lobe infarction (cerebral blindness)
○ Visual hallucinations
● Pupillary abnormalities
○ Tonic pupil
○ Horner syndrome
Fluorescein angiography shows choroidal ischemia (delayed and patchy choroidal filling) in many patients with giant cell arteritis (▶Fig. 20.27).
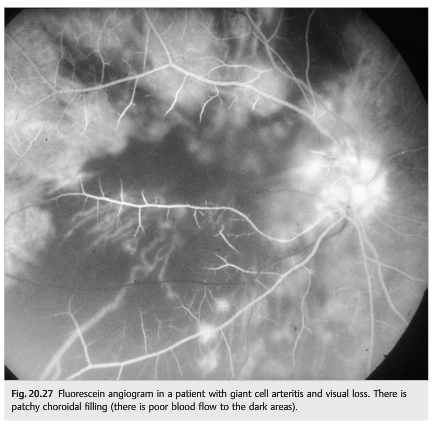
Although nonspecific, this feature is very suggestive of giant cell arteritis in elderly patients with visual loss and normal carotid arteries. The fluorescein angiogram normalizes within 2 weeks of steroid treatment.
Pearls
Ischemic optic neuropathy in giant cell arteritis is often bilaterally sequential and maybe associated with a concurrent choroidal or retinal infarction. The combination of an ischemic optic neuropathy and retinal infarction or choroidal ischemia should strongly suggest the diagnosis of giant cell arteritis.
Ophthalmic Signs Suggesting a High Risk for Giant Cell Arteritis
The following ophthalmic signs are very suggestive of giant cell arteritis and should prompt immediate evaluation and treatment:
● AION with one or more of the following:
○ Severe visual loss
○ A large cup-to-disc ratio (no disc-at-risk for nonarteritic AION)
○ Pale/milky/chalky white optic disc edema acutely
○ Cotton wool spots suggesting associated retinal ischemia
○ Choroidal ischemia
○ Transient visual loss preceding the AION
○ Transient diplopia preceding the AION
○ Headache, orbital or ocular pain
● PION in the absence of prior surgery, severe blood loss, or hypotension—manifests acutely as vision loss with an ipsilateral relative afferent pupillary defect and normal-appearing optic nerve
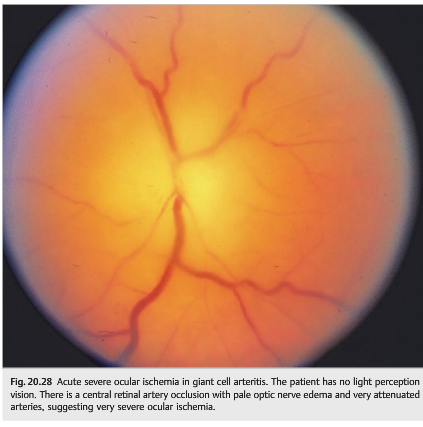
● Any combination of ophthalmic vascular events in close temporal proximity, especially those affecting separate vascular territories (i.e., posterior ciliary and retinal arteries) or affecting both eyes simultaneously or sequentially (▶Fig. 20.28)
● Cilioretinal artery occlusion (especially with AION)
Pearls
In the elderly, the association of very severe visual loss with ocular ischemia and pallid optic nerve head edema acutely is essentially diagnostic of giant cell arteritis. Steroids must be started immediately to prevent visual loss in the fellow eye (intravenous methylprednisolone is started immediately in the emergency room prior to admitting the patient for workup and further treatment).
20.3.2 Diagnosis of Giant Cell Arteritis
● Clinical suspicion (age, clinical manifestations)
○ Ocular manifestations isolated in up to 25% of cases
● Demonstration of biological inflammatory syndrome
○ Erythrocyte sedimentation rate (ESR) elevated—may be normal in up to 20% of cases
○ C-reactive protein (CRP) elevated
○ Low hematocrit
○ Platelet count elevated
○ Fibrinogen elevated
● Temporal artery biopsy (▶Fig. 20.29 and ▶Fig. 20.30)

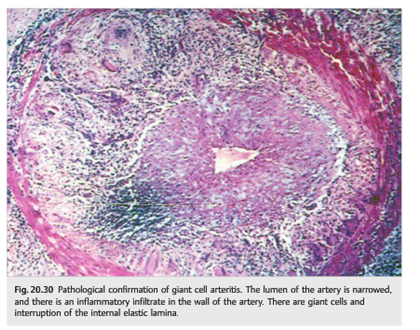
○ Only definite confirmation of the diagnosis
○ Must always be performed
○ False-negative in about 4 to 5% of cases
● Fluorescein angiogram
○ Delayed choroidal filling
○ Useful when diagnosis is uncertain
● Imaging of the aorta and its branches
○ Useful when the diagnosis is uncertain
Superficial temporal artery biopsy is performed under local anesthesia and is a relatively benign procedure. The artery is identified under the skin by either palpation or Doppler ultrasonography. A superficial incision is made along the course of the artery. Blunt dissection allows visualization of an arterial segment long enough to remove at least 2 to 3 cm for pathological examination. The artery is either ligated or cauterized at the proximal and distal ends of the specimen, and the skin is closed. Stitches are removed a week later. Complications are rare and include injury to the frontal branch of the facial nerve (paralysis of the ipsilateral forehead), infection, bleeding, and skin necrosis.
Rheumatologic Criteria for the Diagnosis of Giant Cell Arteritis
The diagnosis of giant cell arteritis requires at least three of these five criteria to be present:
1. Age at disease onset 50 years or older
2. New onset or new type of headache
3. Temporal artery tenderness to palpation or decreased pulsation, unrelated to arteriosclerosis of cervical arteries
4. Elevated sedimentation rate (≥50mm/h) by the Westergren method
5. Abnormal artery biopsy showing vasculitis characterized by a predominance of mononuclear cell infiltration or granulomatous inflammation, usually with multinucleated giant cells.
20.3.3 Treatment
The treatment of giant cell arteritis is urgent and the temporal artery biopsy is often performed after treatment is initiated. Laboratory testing should be done prior to initiating any treatment.
Treatment with steroids cures the arteritis, and the typical pathological signs of giant cell arteritis resolve within a few weeks. Ideally the temporal artery biopsy should be performed within 2 weeks of treatment with steroids.
Giant cell arteritis is exquisitely responsive to steroids. Steroids must be started as soon as the diagnosis is suspected to prevent visual loss (the temporal artery biopsy is done a few days later to confirm the diagnosis). Dose and route depend on the clinical manifestations. These patients need to be treated with steroids until there is no evidence of disease activity (no clinical symptoms and no biological inflammatory syndrome)—the total duration of treatment is at least 1 to 2 years, during which the steroids are slowly tapered. In all cases, careful follow-up with monitoring and treatment of complications of steroid treatment is mandatory.
Systemic forms of giant cell arteritis (polymyalgia rheumatica) usually require only low doses of oral prednisone. Ischemic complications of giant cell arteritis (visual loss) usually require high doses of steroids (1 mg prednisone/kg/d). Intravenous (IV) treatment with methylprednisolone (1g/d for 3 days) followed by oral prednisone (1 mg/kg/d) is often chosen in patients with acute visual loss when there is no contraindication.
As a general rule, the taper should be slow (~ 10mg/mon) so that patients reach 20 mg of prednisone/d after 6 months, and 10 mg of prednisone/d after 1 year. Patients are seen monthly while tapering the prednisone (for neuro-ophthalmic examination, evaluation of side effects, biological markers). Any clinical or biological indication of activity of the disease should result in an increase of the steroids and a slower taper.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.