Questions:
15. What should be measured in all patients with headache?
16. What must be ruled out in all patients with headache?
17. What must be measured in all patients with recurrent, unilateral pain localized around the eye?
18. What lab tests should be done in all patients over age 50 with any headache or facial pain?
19. What should be considered and done when a patient presents with a thunderclap headache?
____________________________________________________
Questions with answers:
15. What should be measured in all patients with headache?
Blood pressure
16. What must be ruled out in all patients with headache?
Papilledema
17. What must be measured in all patients with recurrent, unilateral pain localized around the eye?
Intraocular pressure needs to be measured and detailed ocular examination needs to be performed in patients with recurrent, unilateral pain localized around the eye.
18. What lab tests should be done in all patients over age 50 with any headache or facial pain?
Rule-out cranial arteritis with CRP, ESR, and platelet count.
19. What should be considered and done when a patient presents with a thunderclap headache?
A thunderclap headache is a high-intensity headache of abrupt onset mimicking that of a ruptured cerebral aneurysm. The search for an underlying cause should be immediate, exhaustive, and performed in an emergency department. A thunderclap headache is frequently associated with serious vascular intracranial disorders, particularly subarachnoid hemorrhage, intracerebral hemorrhage, cerebral venous thrombosis, unruptured vascular malformation (mostly aneurysm), arterial dissection (intracranial and extracranial), central nervous system vasculitis, reversible vasoconstriction syndrome, pituitary apoplexy, colloid cyst of the third ventricle, CSF hypotension, and acute sinusitis (particularly with barotrauma).
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
19.5 Evaluation of the Patient with Suspected Secondary Headache or Facial Pain
The type of workup depends primarily on the mode of onset of the pain and available resources (▶Fig. 19.1 and ▶Fig. 19.2). All patients with acute headache or facial pain, or rapidly progressive pain, require an urgent evaluation.
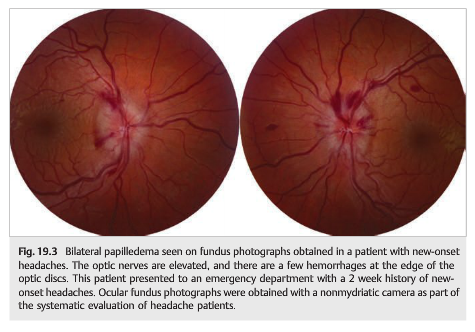
Patients with abnormal clinical examination, with optic nerve head edema (▶Fig. 19.3), or with associated neuro-ophthalmic symptoms or signs also need to be further evaluated. In most cases of long-standing episodic pain suggesting a primary headache or pain disorder with a normal examination (including normal funduscopic evaluation), no further investigation is necessary.
In cases with acute or subacute headache, ancillary investigations are usually obtained in the following order:
1. Blood tests in patients >age 50 (complete blood count, platelet count, erythrocyte sedimentation rate, and C-reactive protein)
2. Head computed tomography (CT) without contrast first to rule out a subarachnoid hemorrhage and screen for hydrocephalus, followed by contrast to screen for mass lesions and meningeal processes or brain magnetic resonance imaging (MRI) with contrast. Depending on the type of headache, computed tomographic angiography(CTA) with contrast may be obtained immediately after the initial head CT without contrast.
3. Lumbar puncture with CSF opening pressure and CSF analysis
4. Brain MRI with contrast if the above investigations are normal.
5. Brain and neck magnetic resonance angiography (MRA) or magnetic resonance venography (MRV) may also be needed, depending on associated symptoms and signs. Dedicated orbital views are necessary if there is an orbital syndrome or if there is unilateral visual loss.
Depending on its availability and on the clinical suspicion, the MRI may replace the head CT, and vascular imaging (with MRA/MRA or CTA) may be obtained initially. The only cause of headache that could be seen on a CT scan and missed by MRI is a subarachnoid hemorrhage, especially during the first week.
6. Cerebral angiography is indicated only in patients with subarachnoid hemorrhage. Arterial dissections, cerebral venous thrombosis, and most aneurysms can usually be diagnosed noninvasively with MRI, MRA, MRV, computed tomographic angiography, or computed tomographic venography.


Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.