Questions:
1. What are the characteristics of a typical migraine aura?
2. What is the longest duration of a typical migraine aura?
3. Does a typical migraine aura develop gradually?
4. What are the characteristics of the most common type of migraine aura?
5. At what point in a migraine with aura attack should vasoconstrictive treatments used to abort the attack be administered (e.g. ergotamine and triptans)?
____________________________________________________
Questions with answers:
1. What are the characteristics of a typical migraine aura?
A typical aura consists of visual and/or sensory and/or speech symptoms with:
1. gradual development, duration no longer than 1 hour
2. a mix of positive and negative features
3. complete reversibility.
2. What is the longest duration of a typical migraine aura?
1 hour
3. Does a typical migraine aura develop gradually?
Yes
4. What are the characteristics of the most common type of migraine aura?
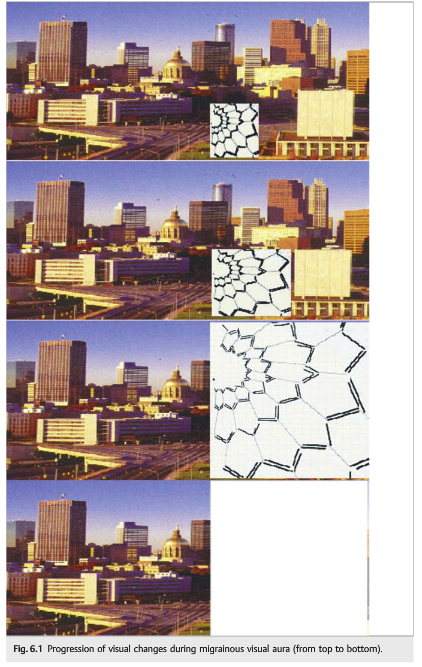
Visual aura is the most common type, often presenting as a fortification spectrum (zigzag figure near the point of fixation that may gradually spread right or left and assuming a laterally convex shape with an angulated scintillating edge leaving variable degrees of absolute or relative scotoma in its wake). A progressively enlarging scotoma without positive phenomena may occur.
5. At what point in a migraine with aura attack should vasoconstrictive treatments used to abort the attack be administered (e.g. ergotamine and triptans)?
They should not be used during the aura. The patients should be instructed to wait until the aura has resolved to take such medications.
6. What are the 2 categories of trigeminal neuralgia (tic douloureux)?
1. Classic Trigeminal Neuralgia
2. Symptomatic Trigeminal Neuralgia
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
19 Diagnosis of Headache and Facial Pain
Headache and facial pain accompany or reveal many neuro-ophthalmic disorders. The diagnosis of the cause of headache and facial pain is based on clinical history. In particular, the mode of onset of pain and its temporal profile are of great importance. These characteristics are the key indicators of whether the pain is due to a benign headache, a facial pain syndrome, or a neuro-ophthalmic disorder.
19.1 Clinical Diagnosis of Headache and Facial Pain
The clinical diagnosis of headache and facial pain depends on characterization of the mode of onset of pain (▶Fig. 19.1). For example, an acute, recent onset is usually related to an emergency, whereas episodic pain, with pain-free intervals between attacks, is usually related to a benign, primary headache or facial pain disorder. Progressive, permanent pain over a few days or a few weeks is usually related to an intracranial space-occupying lesion. A long-standing, chronic headache is usually related to a benign process.
19.1.1 Other Characteristics of the Pain
The following characteristics of the pain guide further evaluation:
● Location of pain (diffuse, hemicrania, periorbital, occipital, or cervical)
● Side of pain (unilateral, alternating, or bilateral)
● Type of pain (dull, constant, or throbbing)
● Duration of pain (without treatment)
● Severity of pain (using a scale from 1 to 10, particularly considering its impact on activities)
● Frequency of episodes (per day, week, or month)
● Temporal profile (age of onset, recent worsening, and progressive)
● Precipitating factors
● Prodromes (i.e., early symptoms preceding onset)
● Associated symptoms and signs (nausea, vomiting, photophobia, tearing, ocular redness, visual loss, Horner syndrome, diplopia, and sleep apnea)
● Treatments tried and their efficacy
19.2 Clinical Evaluation of the Patient with Headache/Facial Pain
Clinical evaluation should include a detailed neurologic examination, including cranial nerve examination; a funduscopic examination looking for disc edema, which would reveal papilledema from raised intracranial pressure, and spontaneous venous pulsations, which would suggest normal intracranial pressure; palpation of the temporal arteries (for patients > age 50); blood pressure and temperature; and a general physical examination.
In most cases, the cause of headache or facial pain is identified at this point. The International Headache Society (IHS) has proposed a classification of headaches according to their underlying mechanisms. It is important to recognize the primary headaches or facial pain (usually benign disorders) and differentiate them from the secondary headaches and facial pain, which reveal an underlying disease. Further investigations are obtained when a secondary cause of pain is suspected (▶Fig. 19.2).
Pearls
● Blood pressure should be checked in all headache patients (acute or chronic).
● Examination of the ocular fundus is required in all patients presenting with chronic or new-onset headaches.
● The presence of optic nerve head edema suggests raised intracranial pressure.
● Giant cell arteritis should be considered in all patients > age 50 who present with any type of headache or facial pain.
● Intraocular pressure and detailed ocular examination need to be performed in patients with recurrent, unilateral pain localized around the eye.
19.3 Classification of Headache and Facial Pain
The following classification is adapted from the Headache Classification Subcommittee of the International Headache Society. International Classification of Headache Disorders, 3rd ed. (ICHD-III). Cephalalgia 2013;33(9):629–808. In each subgroup, we have detailed only disorders that may present with neuro-ophthalmic symptoms and signs.
a) Primary headaches
● Migraine
○ Migraine with visual aura
● Tension-type headache and new daily persistent headache
● Cluster headache and other trigeminal autonomic cephalalgias
○ Cluster headache (episodic and chronic)
○ Paroxysmal hemicrania (episodic and chronic)
○ Short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT)
● Other primary headaches
○ Hemicrania continua


b) Secondary headaches
● Headaches attributed to head and/or neck trauma
● Headaches attributed to cranial or cervical vascular disorders
○ Ischemic and hemorrhagic strokes
○ Unruptured and ruptured vascular malformations (aneurysm, arteriovenous malformation, dural arteriovenous fistula, cavernous angioma, Sturge-Weber syndrome)
○ Giant cell arteritis
○ Central nervous system vasculitis
○ Carotid or vertebral artery dissection
○ Reversible vasoconstriction syndrome
○ Cerebral venous thrombosis
○ Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)
○ Mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS)
○ Pituitary apoplexy
● Headaches attributed to nonvascular intracranial disorders
○ High cerebrospinal fluid (CSF) pressure
○ Low CSF pressure
○ Meningeal processes
○ Intracranial neoplasms
○ Chiari malformation
● Headaches attributed to a substance or its withdrawal
● Headaches attributed to infection
○ Meningitis, encephalitis, intracranial abscess
● Headaches attributed to disorders of homeostasis
○ Hypoxia
○ High altitude
○ Sleep apnea
○ Dialysis
○ Arterial hypertension
○ Hypoglycemia
● Headaches or facial pain attributed to disorders of the cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial or cranial structures
○ Acute glaucoma
○ Refractive errors
○ Heterophoria or heterotropia
○ Ocular inflammatory disorders (uveitis, scleritis, orbital inflammation, optic neuritis)
● Headaches attributed to psychiatric disorder
c) Cranial neuralgias, central and primary facial pain, other headaches
● Cranial neuralgias and central causes of facial pain
○ Trigeminal neuralgia (classic, symptomatic)
○ Nasociliary neuralgia
○ Supraorbital neuralgia
○ Optic neuritis
○ Herpes zoster
● Other headaches, cranial neuralgia, central or primary facial pain
Pearls
Thunderclap headache is a high-intensity headache of abrupt onset mimicking that of a ruptured cerebral aneurysm. The search for an underlying cause should be immediate (and performed in an emergency department) and exhaustive. Thunderclap headache is frequently associated with serious vascular intracranial disorders, particularly subarachnoid hemorrhage, intracerebral hemorrhage, cerebral venous thrombosis, unruptured vascular malformation (mostly aneurysm), arterial dissection (intra- and extracranial), central nervous system vasculitis, reversible vasoconstriction syndrome, pituitary apoplexy, colloid cyst of the third ventricle, CSF hypotension, and acute sinusitis (particularly with barotrauma).
Primary thunderclap headache should be the diagnosis only when all organic causes have been excluded.
19.3.1 Diagnostic Criteria for Migraine without Aura
The following information is based on ICHD-III Diagnostic Criteria for Migraine.
Description
Migraine is defined as a recurrent headache disorder with attacks lasting 4 to 72 hours. Typical characteristics of the headache are unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity, and association with nausea and/or photophobia.
Diagnostic Criteria
a) At least five attacks fulfilling criteria B to D
b) Headache attacks lasting 4 to 72 hours (untreated or unsuccessfully treated)
c) Headache has at least two of the following characteristics:
● Unilateral location
● Pulsating quality
● Moderate or severe intensity
● Aggravation by or causing avoidance of routine physical activity (e.g., walking or climbing stairs)
d) During headache, at least one of the following:
● Nausea and/or vomiting
● Photophobia and phonophobia
e) Not attributable to another disorder
19.3.2 Diagnostic Criteria for Migraine with Aura
The following information is based on ICHD-II Diagnostic Criteria for Migraine with Aura.
Description
Migraine with aura is defined as a recurrent headache disorder with attacks of reversible neurologic symptoms, usually developing gradually over 5 to 20 minutes and lasting for<60 minutes. Headaches with the features of migraine without aura usually follow the migraine with aura symptoms. Less commonly, headaches without the features of migraines or no headaches follow.
Diagnostic Criteria
a) At least two attacks fulfilling criteria B and C of migraine headache
b) Migraine fulfilling criteria for typical aura
c) Not attributed to another disorder
A typical aura consists of visual and/or sensory and/or speech symptoms. Gradual development, duration no longer than 1 hour, a mix of positive and negative features, and complete reversibility characterize the aura.
Visual aura is the most common type, often presenting as a fortification spectrum(zigzag figure near the point of fixation that may gradually spread right or left and assuming a laterally convex shape with an angulated scintillating edge leaving variable degrees of absolute or relative scotoma in its wake). A progressively enlarging scotoma without positive phenomena may occur (▶Fig. 6.1, ▶Fig. 11.2).
Pearls
Some of the treatments used to abort migrainous headaches are vasoconstrictors and should not be used during the aura. The patients should be instructed to wait until the aura has resolved to take such medications (e.g., ergotamine and triptans).

Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.