Questions:
1. What is the difference in the meaning of functional, nonphysiologic, and nonorganic visual loss?
2. What is the only way to confirm the diagnosis of nonorganic visual loss?
3. Is it common for nonorganic symptoms to be superimposed on organic disease?
4. In a patient complaining of substantial visual loss in only one eye, and no history of amblyopia and a normal standard eye examination, what 4 tests that can be used to determine if the vision loss is inorganic?
5. What are 2 techniques for the Fogging test for functional vision loss?
6. How is the horizontal prism shift test performed?
7. How is the vertical prism dissociation test performed?
8. When the complaint is “No Light Perception or Hand Motion Vision in Both Eyes”, what 5 tests that can be used to determine if that the vision loss is inorganic?
9. What visual field findings are common in nonorganic visual loss?
____________________________________________________
Questions with answers:
1. What is the difference in the meaning of functional, nonphysiologic, and nonorganic visual loss?
None, they all include the entire spectrum of this condition: malingering, secondary gain (financial or psychological), hysteria, Munchausen syndrome, etc.
2. What is the only way to confirm the diagnosis of nonorganic visual loss?
The only way to confirm that the symptoms and signs are nonorganic is to prove that visual function is normal.
3. Is it common for nonorganic symptoms to be superimposed on organic disease?
Yes
4. In a patient complaining of substantial visual loss in only one eye, and no history of amblyopia and a normal standard eye examination, what 4 tests that can be used to determine if that the vision loss is inorganic?
1. Fogging
2. Stereopsis
3. Horizontal prism shift test
4. Vertical prism dissociation test
5. What are 2 techniques for the Fogging test for functional vision loss?
1. This can be done by placing a plus lens (≥+5.00D over the normal refractive correction) in front of the good/unaffected eye and a lens with minimal power over the affected eye. The patient is then asked to read the chart with both eyes. The patient may not realize that the unaffected eye is fogged and a patient with functional monocular visual loss often reads well with the “affected” eye.
2. Paired cylinders can also be used. A plus cylinder and a minus cylinder of the same power are placed in parallel in front of the good/unaffected eye. While the patient reads the chart, the axis on one cylinder is rotated 10-15 degrees to fog the good/unaffected eye. If the patient continues to read the chart successfully, they are revealing adequate vision in the “affected” eye.
6. How is the horizontal prism shift test performed?
A normal prism shift test requires binocular vision. Ask the patient to look at the Snellen chart showing smaller letters than what the patient claims to be able to see in the bad eye. Place a 4-diopter prism (base in) in front of the “bad” eye. If the patient truly sees the letters with both eyes, then a compensatory movement of both eyes toward the apex of the prism is followed by a convergence movement of the good eye as the patient tries to suppress diplopia. If vision is organically reduced in the bad eye, there will be no compensatory eye movement.
7. How is the vertical prism dissociation test performed?
A 4 diopter prism base-down is placed before the good eye while observing a single line on the visual acuity chart. If the patient has symmetrical vision in both eyes, 2 images will be seen. If the patient is only able to see the letters with the “good” eye, then only 1 image should be seen.2
8. When the complaint Is “No Light Perception or Hand Motion Vision in Both Eyes”, what 5 tests that can be used to determine if that the vision loss is inorganic?
1. Surprise the patient- unexpected actions from the examiner can elicit a surprise response from the patient.
2. Test proprioception: truly blind patients have no difficulty performing tests that appear to require vision but are actually proprioception tasks (e.g., “Bring the tips of your index fingers together”.
3. Test for optokinetic nystagmus: a positive response indicates that visual acuity is at least 20/400 vision in the tested eye.
4. The mirror test is helpful in patients with “no light perception” or “light perception” vision. A patient with nonorganic visual loss will be unable to avoid eye movements following his or her own image in a mirror that is held close to the face and rocked back and forth and up and down.
5. Visual evoked potentials: normal visual evoked responses indicate intact visual pathways for central vision however abnormal visual evoked responses can be from defocusing, poor fixation, and poor effort.
9. What visual field findings are common in nonorganic visual loss?
Goldmann automated visual fields show generalized constriction, the size of the visual field does not vary with the size of the stimulus, and/or isopters may be overlapping, reversed, or spiraled.
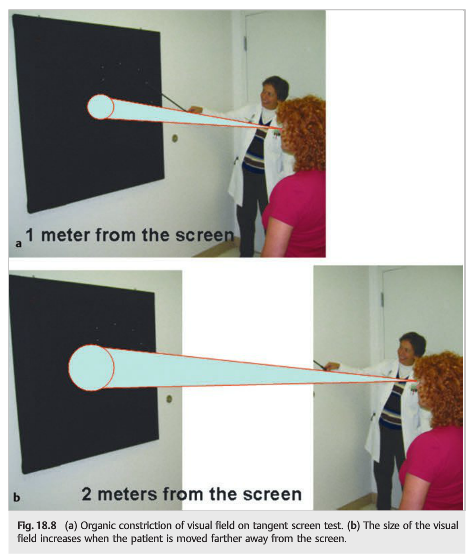
Tangent screen visual fields will often have the same absolute size (tubular or gun-barrel field) when the test is performed at two different distances from the screen (usually 1 and 2 meters) while maintaining the same ratio of target size to target distance (i.e., larger target at a further distance).
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme1
18 Nonorganic Neuro-ophthalmic Symptoms and Signs
Nonorganic visual symptoms and signs – patients’ visual complaints that are not supported by clinical examination – are common in neuro-ophthalmology. Classic nonorganic symptoms and signs include unilateral or bilateral visual loss, which ranges from blurred vision to complete blindness; peripheral visual field loss, which is usually visual field constriction; monocular diplopia; spasm of the near reflex; voluntary nystagmus; pharmacologic dilation of one or both pupils; disturbance of accommodation; and voluntary ptosis and blepharospasm.
This chapter discusses warning signs that visual symptoms and signs are nonorganic and offers examination strategies to confirm their inorganic nature.
18.1 Types of Visual Symptoms and Signs
The neuro-ophthalmologist is often in the position of showing that the visual system is actually normal and that these symptoms and signs are associated with various psychiatric disorders that present with nonorganic (functional or psychogenic) neuro-ophthalmic symptoms and signs.
Most patients in these cases are found to have the following:
● Nonspecific visual symptoms that are part of a depressive or anxiety disorder (e.g., chronic eye pain, photosensitivity, or asthenopia)
● Visual symptoms and signs that are part of a conversion disorder, hypochondriasis, or somatization disorder syndrome (in these cases, the patient may not be aware of the nonorganic nature of the symptoms)
● Visual symptoms and signs that are part of a factitious disorder (Munchausen Syndrome)
● Visual symptoms and signs that are being feigned to seek compensation or disability(malingering)
● Visual symptoms and signs that are being used to seek medical help and escape from a difficult situation (if abuse is suspected, patients should be admitted for further evaluation)
Psychiatric evaluation should be suggested when an underlying psychiatric disorder is suspected.
18.2 Examination Strategies to Confirm That Symptoms and Signs Are Nonorganic
The only way to confirm that the symptoms and signs are nonorganic is to prove that visual function is normal during the examination. Specific examination strategies can be used, but only if the visual symptoms and signs are suspected to be nonorganic prior to the examination.
Nonorganic visual symptoms and signs are usually suspected early during the interaction with the patient. A discrepancy between the patient’s complaints and the patient’s activities in the waiting room should raise a red flag. Another tip is that patients claiming nonorganic visual loss often wear sunglasses, even in the examination room.
Patients with true visual loss tend to look at the examiner during the interview and examination, whereas patients with nonorganic visual loss tend to look in other directions and often pretend to have difficulty following instructions during the examination.
Pearls
The diagnosis of nonorganic visual loss should be made cautiously and only when the examiner is able to prove normal vision. It is common to see patients with true organic disease but superimposed nonorganic symptoms (e.g., a patient with true visual loss from brain injury may worsen his complaints to avoid having to return to work, or the same patient may have secondary depression and somatization).
18.2.1 When the Complaint Is Visual Loss
1. Observe the patient walking without help from the waiting room into the examination room.
2. Visual acuity testing:
● Start at the very bottom of the Snellen chart (at the 20/10 line) and encourage the patient to see the letters, emphasizing that the size of the letters doubles at each line. Most patients read the letters by the time you reach the 20/30 or 20/40 line.
● Attempt a fake refraction (by placing neutral lenses in front of the tested eye); it often improves vision, particularly in children.
● “Magic drop” test: emphasize that the drops you are placing in the eyes (artificial tears) are going to improve the vision temporarily and help you understand the mechanism of vision loss (this is particularly helpful in children).
When the Complaint Is Substantial Visual Loss in One Eye Only
If the patient has clear ocular media, no major refractive error determined by retinoscopy, and no history of amblyopia, try the following:
1. Check for normal pupillary responses (absence of relative afferent pupillary defect), which suggest that unilateral visual loss is not related to an optic neuropathy or severe retinopathy.
2. Test stereovision to objectively measure visual acuity in both eyes (equal vision in both eyes is required for stereopsis) (▶Fig. 18.1; ▶Table 18.1).
3. Fog the good eye with plus lenses while measuring visual acuity with both eyes open so that only the “bad eye” sees (the patient is usually not aware of which eye is being tested).
4. Perform a prism shift test. A normal prism shift test requires binocular vision. Ask the patient to look at the Snellen chart showing small letters (smaller than what the patient claims to be able to see in the bad eye). Place a 4-diopter prism (base in) in front of the alleged bad eye. If the patient truly sees the letters with both eyes, then a compensatory movement of both eyes toward the apex of the prism is followed by a convergence movement of the good eye as the patient tries to suppress diplopia. If Vision is organically reduced in the bad eye, there will be no compensatory eye movement.

When the Complaint Is No Light Perception or Hand Motion Vision in Both Eyes
1. Surprise the patient: Unexpected actions from the examiner can elicit a surprise response from the patient.
2. Test proprioception: Truly blind patients have no difficulty performing tests that appear to require vision but are actually proprioception tasks (e.g., “Look at your hand,” “Bring the tips of your index fingers together,” and “Sign your name”) (▶Fig. 18.2).

3. Test for optokinetic nystagmus: A positive response indicates vision of at least 20/400 vision in the tested eye (▶Fig. 18.3).

4. Perform the mirror test: The mirror test is helpful in patients with “no light perception” or “light perception” vision. Patients with nonorganic visual loss will be unable to avoid eye movements following their own image in a mirror that is held close to their face and rocked back and forth and up and down (▶Fig. 18.4). The optokinetic test and the mirror test can be performed with both eyes open if the patient claims complete bilateral blindness. It should be performed with the good eye patched if the patient claims blindness in only one eye.

5. Use visual evoked potentials: Normal visual evoked responses indicate intact visual pathways for central vision. Abnormal visual evoked responses do not prove organic visual loss (they can be abnormal from defocusing, poor fixation, and poor effort).
18.2.2 When the Complaint Is Constriction of Visual Fields
Constricted visual fields are seen with automated and Goldmann visual fields. There is generalized constriction, and on Goldmann visual fields, the size of the visual field does not vary with the size of the stimulus, or isopters may be overlapping, reversed, or spiraled (▶Fig. 18.5).
1. Test the confrontation visual field: Ask the patient to mime what you are doing in the peripheral vision of one or both eyes (▶Fig. 18.6).
● Tell the patient that you are testing coordination, not vision.
● Next, quickly tell the patient to “hold up your hands,” “show me two fingers,” then “do this” (and do something with your hands—wave or make fists—without saying aloud what you are doing).
● Often, a patient will follow along even though the patient says he or she cannot see your hands (this is a sort of “Simon Says” game).


2. Test tangent screen visual field: With nonorganic constricted visual field, the size of the visual field does not physiologically increase when the distance at which the visual field is tested increases (tubular visual field) (▶Fig. 18.7, ▶Fig. 18.8).

18.2.3 When the Complaint Is Monocular Diplopia
Patients with ocular misalignment have binocular diplopia (diplopia resolves with closing either eye).
When diplopia does not resolve when closing either eye, the diplopia is monocular.
In most cases, there is no true diplopia, but rather ghosting or distortion of images, which improves or resolves by looking through a pinhole (monocular diplopia of optical origin).
Have the patient draw what he or she sees: True monocular diplopia (when two separate and equal images of an object are seen by one eye only) is almost always non-organic.
References:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
2. The Monocular Vertical Prism Dissociation Test
Am J Ophthalmol. 2004 Jan;137(1):135-7. Karl C Golnik, Andrew G Lee, Eric R Eggenberger
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.