Questions:
28. What may patients with peripheral facial palsy ultimately develop?
29. What should be suspected in all patients with hemifacial spasm?
30. What test should be done in all patients with hemifacial spasm?
31. What are 4 causes of blepharospasm?
32. A patient has blepharospasm accompanied by dystonic movements of the lower face or neck. What is the diagnosis?
33. Is eyelid pain to be expected in a patient with blepharospasm?
34. How is a patient with blepharospasm likely to describe their eyelid pain?
35. What is the treatment of choice in patients with chronic blepharospasm?
36. What is the treatment of choice in patients with hemifacial spasm?
37. What is the mechanism of action of botulinum toxin injections?
38. Does botulinum toxin injection relieve the crampy pain of a patient with blepharospasm?
39. In a patient with blepharospasm, does botulinum toxin injection relieve the eyelid spasms immediately?
____________________________________________________
Questions with answers:
28. What may patients with peripheral facial palsy ultimately develop?
Hemifacial spasm (involuntary contraction of the hemiface, often predominating around the eye).
29. What should be suspected in all patients with hemifacial spasm?
A compressive lesion of the facial nerve.
30. What test should be done in all patients with hemifacial spasm?
An MRI of the brain with contrast.
31. What are 4 causes of blepharospasm?
1. Ocular surface irritation (severe dry eye syndrome)
2. Essential blepharospasm (idiopathic dystonia)
3. Parkinson syndrome
4. Pontine lesions
32. A patient has blepharospasm accompanied by dystonic movements of the lower face or neck. What is the diagnosis?
Oromandibular dystonia (Meige syndrome)
33. Is eyelid pain to be expected in a patient with blepharospasm?
Yes
34. How is a patient with blepharospasm likely to describe their eyelid pain?
As cramps of the involved muscles.
35. What is the treatment of choice in patients with chronic blepharospasm?
Local injections of botulinum toxin in the orbicularis oculi.
36. What is the treatment of choice in patients with hemifacial spasm?
Local injections of botulinum toxin in the facial muscles responsible for the spasms.
37. What is the mechanism of action of botulinum toxin injections?
Botulinum toxin blocks the release of acetylcholine at the neuromuscular junction, thereby rendering the muscle unable to contract for a period of approximately three months.
38. Does botulinum toxin injection relieve the crampy pain of a patient with blepharospasm?
Yes, and the effect on pain is immediate.
39. In a patient with blepharospasm, does botulinum toxin injection relieve the eyelid spasms immediately?
No, the effect on the spasms is usually delayed by a few days and usually lasts about 10 weeks.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
17.4 Peripheral Facial Weakness
Peripheral facial weakness results in decreased closure of the eyelid and a larger palpebral fissure. When the Bell phenomenon is preserved, the cornea is still partially protected during sleep (▶Fig. 17.24).

When there is complete facial palsy and no Bell Phenomenon, the cornea is exposed (▶Fig. 17.25).

Complications of incomplete eye closure include ocular surface irritation (pain, redness, and visual loss), corneal exposure, and risk of corneal infection and perforation (▶Fig. 17.26).

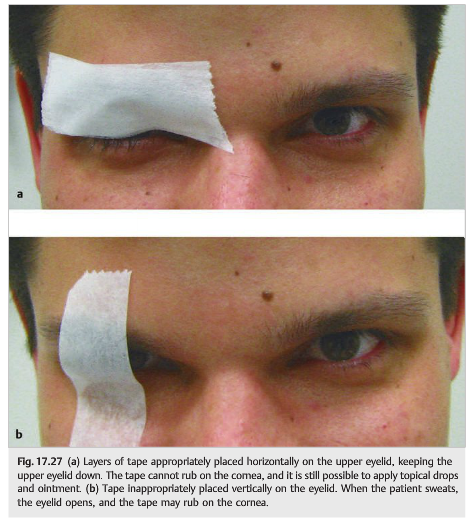
These patients need to be evaluated by an ophthalmologist. Artificial tears and lubricant ointment need to be applied to the cornea every few hours. If the eye closure is incomplete, then the eyelid may be temporarily closed by placing tape horizontally on the upper lid (▶Fig. 17.27).
When the cornea is exposed, the upper and lower eyelids can be sewn together to keep the eye closed and the cornea protected. This procedure is called a tarsorrhaphy, which can be performed at bedside (▶Fig. 17.28).

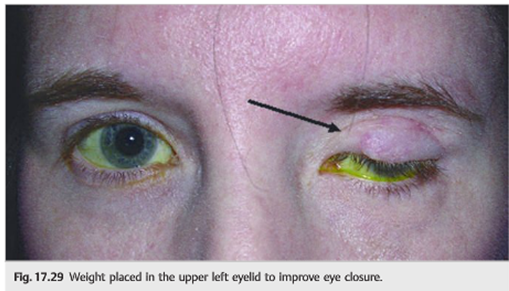
If the facial weakness does not improve, various procedures can be performed later to improve eye closure (▶Fig. 17.29).
Patients with a peripheral facial palsy may ultimately develop hemifacial spasm (involuntary contraction of the hemiface, often predominating around the eye). This occurs more commonly when there is a compressive lesion of the facial nerve.
Pearls
All patients with hemifacial spasm need magnetic resonance imaging (MRI) of the brain, with contrast, looking for a lesion compressing the facial nerve.
17.5 Abnormal Blinking
Regular blinking, which is defined as 20 to 30 blinks per minute, keeps the eye from drying out by evenly distributing the lacrimal fluid and glandular secretions.
17.5.1 Decreased Blinking
Decreased spontaneous blinking is common in patients with Parkinson syndromes.
Patients with facial weakness also have decreased (and often incomplete) blinking.
17.5.2 Blepharospasm
Blepharospasm, or involuntary intermittent bilateral eyelid closure, ranges from an increased blink rate to severe, sustained spasms of the orbicularis oculi. Spasms are worse with wind, sun, light, and stress.
Causes of blepharospasm include the following:
● Ocular surface irritation (severe dry eye syndrome)
● Essential blepharospasm (idiopathic dystonia)
● Parkinson syndrome
● Pontine lesions
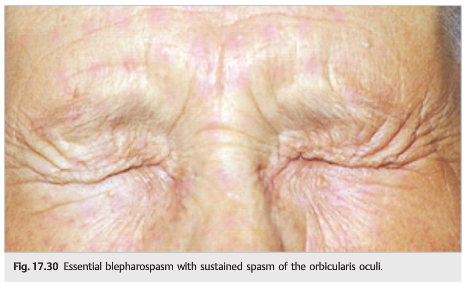
Blepharospasm accompanied by dystonic movements of the lower face or neck (oromandibular dystonia) is called Meige syndrome. Severe spontaneous eyelid closure from blepharospasm can result in functional blindness and severe disability. Some patients cannot keep their eyes open long enough to cross a street. They cannot read and cannot drive. Pain is common (described as cramps of the involved muscles) (▶Fig. 17.30).
The treatment of choice in patients with blepharospasm or hemifacial spasm is local subcutaneous injections of botulinum toxin. Botulinum toxin is injected subcutaneously in the muscles responsible for the spasms (in the orbicularis oculi and other facial muscles if necessary). Botulinum toxin blocks the release of acetylcholine at the neuromuscular junction, thereby rendering the muscle unable to contract for a period of approximately 3 months. The effect on pain is immediate. The effect on the spasms is usually delayed by a few days and lasts several weeks. The injections are repeated every few months. Ocular lubrication is also important.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.