\Questions:
20. What should be ruled out in all cases of ptosis?
21. What are 8 causes of pseudoptosis?
22. What does a show of sclera between the upper eyelid and limbus suggest?
23. What are the 3 categories of eyelid retraction?
24. What are the 3 most common causes of lid retraction?
25. What are 5 causes of mechanical lid retraction?
26. What are 2 causes of myogenic lid retraction?
27. What are 6 causes of neurogenic lid retraction?
____________________________________________________
Questions with answers:
20. What should be ruled out in all cases of ptosis?
Pseudoptosis
21. What are 8 causes of pseudoptosis?
1. Dermatochalasis
2. Contralateral lid retraction
3. Contralateral peripheral facial palsy
4. Duane syndrome
5. Microphthalmos
6. Enophthalmos
7. Voluntary ptosis
8. Blepharospasm
22. What does a show of sclera between the upper eyelid and limbus suggest?
Eyelid retraction
23. What are the 3 categories of eyelid retraction?
1. Mechanical
2. Myogenic
3. Neurogenic
24. What are the 3 most common causes of lid retraction?
1.Thyroid eye disease
2. Dorsal midbrain syndrome (Collier sign)
3. Contralateral ptosis
25. What are 5 causes of mechanical lid retraction?
1. Proptosis
2. High myopia (pseudoproptosis)
3. Ocular or orbital surgery
4. Eyelid scarring
5. Contralateral ptosis
26. What are 2 causes of myogenic lid retraction?
1. Thyroid eye disease
2. Congenital anomaly
27. What are 6 causes of neurogenic lid retraction?
1. Dorsal midbrain syndrome (Collier’s sign)
2. Marcus Gunn jaw winking
3. Aberrant regeneration of the third nerve
4. Third nerve palsy with cyclic spasms
5. Neuromyotonia involving the third nerve
6. Facial nerve paresis
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
17.2.3 Pseudoptosis
In all cases of ptosis, pseudoptosis needs to be ruled out (▶Fig. 17.17 and Fig. 17.18).
Causes of pseudoptosis include the following:
● Dermatochalasis
● Contralateral lid retraction
● Contralateral peripheral facial palsy
● Duane syndrome
● Microphthalmos
● Enophthalmos
● Voluntary ptosis
● Blepharospasm
17.3 Eyelid Retraction
Eyelid retraction is diagnosed when sclera is seen between the lower edge of the upper eyelid and the limbus (edge of the iris).

Causes of lid retraction can be mechanical, myogenic, or neurogenic. The three most common causes of lid retraction are thyroid eye disease, dorsal midbrain syndrome (Collier sign), and contralateral ptosis.
Causes of lid retraction include the following:
● Mechanical
○ Proptosis
○ High myopia (pseudo proptosis)
○ Ocular or orbital surgery
○ Eyelid scarring
○ Contralateral ptosis
● Myogenic
○ Thyroid eye disease
○ Congenital
● Neurogenic
○ Dorsal midbrain syndrome (Collier sign)
○ Marcus Gun jaw winking
○ Aberrant regeneration of the third nerve
○ Third nerve palsy with cyclic spasms
○ Neuromyotonia involving the third nerve
○ Facial nerve paresis
Lid retraction from thyroid eye disease is usually bilateral and is often associated with lid lag in downgaze (▶Fig. 17.19,▶Fig. 17.20,▶Fig. 17.21).
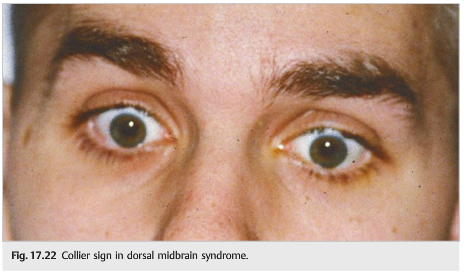
Pretectal eyelid retraction (Collier sign) is observed in the dorsal midbrain (Parinaud) syndrome (▶Fig. 17.22). It is usually accompanied by up gaze paresis and convergence–retraction nystagmus.


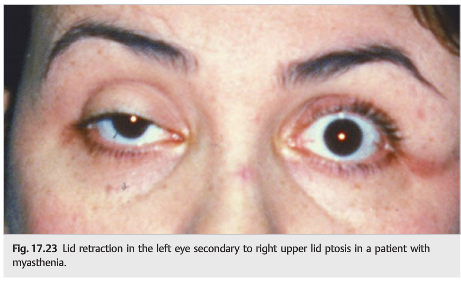
Patients with unilateral ptosis tend to raise their eyebrows to compensate for their ptosis (they use their frontalis muscles more). This may result in lid retraction in the normal fellow eye (▶Fig. 17.23). The examiner should raise the ptotic lid to observe spontaneous resolution of the lid retraction.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.Please send feedback, questions, and corrections to tcooper@stanford.edu