Questions:
13. What diagnosis is most likely when a patient has acquired nystagmus with positional vertigo?
14. What is the most important goal in the evaluation of central nystagmus?
15. Which patterns of jerk nystagmus have localizing value?
16. Which patterns of pendular nystagmus have localizing value?
17. What is downbeat nystagmus?
18. What is upbeat nystagmus?
19. What is periodic alternating nystagmus?
20. What is rebound nystagmus?
21. What is Brun nystagmus?
22. What is dissociated jerk nystagmus?
23. What is acquired pendular nystagmus?
24. What is seesaw nystagmus?
____________________________________________________
Questions with answers:
13. What diagnosis is most likely when a patient has acquired nystagmus with positional vertigo?
Benign paroxysmal positional vertigo.
In this condition paroxysmal vertigo occurs only in certain positions. When the Dix–Hallpike maneuver is performed, nystagmus is seen. Most patients have benign paroxysmal positional vertigo (BPPV) from a peripheral lesion, usually canalolithiasis or cupulolithiasis in the posterior semicircular canal. BPPV does not respond well to medications but may have a long-term favorable response to numerous maneuvers aimed at dislodging the debris from the posterior semicircular canal. Positional vertigo may also occur with central nervous system disease.
14. What is the most important goal in the evaluation of central nystagmus?
The most important goal of the evaluation is to identify those patterns of nystagmus that have a localizing value.
15. Which patterns of jerk nystagmus have localizing value?
1. Downbeat
2. Upbeat
3. Periodic alternating
4. Brun
5. Dissociated jerk.
16. Which patterns of pendular nystagmus have localizing value?
1. Monocular (often vertical) = visual loss
2. Seesaw = parasellar lesions and septo-optic dysplasia
3. Oculopalatal myoclonus = Mollaret triangle (connecting red nucleus to inferior olive and dentate nucleus,
4. Oculomasticatory myorhythmia = Whipple disease).
17. What is downbeat nystagmus?
Downbeat nystagmus is a type of jerk nystagmus, with the fast phase downward in the primary position. The nystagmus decreases in upgaze and worsens in downgaze; it is usually most prominent in lateral gaze and downgaze. Oscillopsia is usually prominent because the nystagmus is present in primary position and in down-gaze, the preferred reading position. Downbeat nystagmus is caused by lesions at the cervicomedullary junction, foramen magnum, vestibulo cerebellum, and medulla. It is commonly seen in cerebellar degenerations; paraneoplastic syndromes; Chiari malformation; encephalitis; trauma; hypomagnesemia; thiamine deficiency; B12 deficiency; and toxicity with lithium, alcohol, amiodarone, toluene, phenytoin, and carbamazepine.
18. What is upbeat nystagmus?
Upbeat nystagmus is a type of jerk nystagmus with the fast phase upward. It often worsens in upgaze. It may be caused by lesions of the medulla, cerebellar vermis, and midbrain and is commonly seen in Wernicke encephalopathy and encephalitis.
19. What is periodic alternating nystagmus?
Periodic alternating nystagmus (PAN) is a type of horizontal jerk nystagmus that alternates direction in primary position (i.e., jerk nystagmus to the right for about 60 to 90 seconds, which diminishes, only to begin beating to the left for another 60 to 90 seconds). Patients may have a periodic alternating head turn to minimize the nystagmus. Oscillopsia is usually present. PAN is caused by lesions of the cerebellum, particularly the nodulus and uvula, and by lesions of the cervicomedullary junction. It is commonly seen in multiple sclerosis, cerebellar degenerations, Chiari malformations, trauma, hepatic encephalopathy, and albinism, as well as with use of anticonvulsants and lithium. It is responsive to baclofen.
20. What is rebound nystagmus?
Rebound nystagmus is seen in some patients with gaze-evoked nystagmus. It is the reversal of jerk nystagmus direction after sustained eccentric gaze. Rebound nystagmus is caused by cerebellar disorders and lesions of the medulla (in the region of the nucleus prepositus hypoglossi and medial vestibular nucleus).
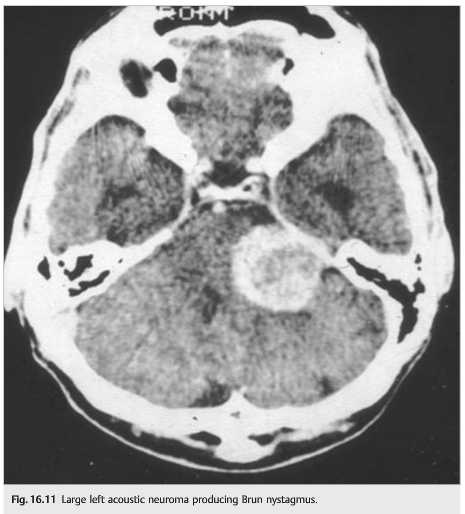
21. What is Brun nystagmus?
Brun nystagmus is a combination of unilateral peripheral vestibular nystagmus from an eighth nerve tumor and gaze-paretic central nystagmus as the tumor compresses the pons. It is characterized by high-frequency, low-amplitude nystagmus on looking away from the lesion, beating in the direction of gaze (due to the vestibular lesion), and low-frequency, high-amplitude horizontal nystagmus on looking toward the lesion, beating in the direction of gaze (due to defective gaze holding). Brun nystagmus is caused by large tumors in the cerebellopontine angle.
Video: http://morancore.utah.edu/section-05-neuro-ophthalmology/bruns-nystagmus/
22. What is dissociated jerk nystagmus?
Dissociated jerk nystagmus refers to nystagmus that is different in the two eyes. The most common cause is internuclear ophthalmoplegia (adduction deficit associated with a contralateral abducting nystagmus).
23. What is acquired pendular nystagmus?
One of the most common types of nystagmus is acquired pendular nystagmus, which is visually disabling because of severe oscillopsia. It most commonly is caused by multiple sclerosis. Oscillopsia may improve with gabapentin, memantine, clonazepam, or valproic acid.
24. What is seesaw nystagmus?
Seesaw nystagmus is defined as pendular nystagmus with elevation and intorsion of one eye simultaneous with depression and extorsion of the other eye, followed by a reversal of the cycle, so that the eyes move like a seesaw. Seesaw nystagmus produces very disabling oscillopsia that responds poorly to any treatment. It is most often caused by parasellar lesions and may be seen with pituitary tumors, craniopharyngiomas, septo-optic dysplasia, and brainstem lesions (especially in the midbrain).
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
16.1.1 Patient Evaluation
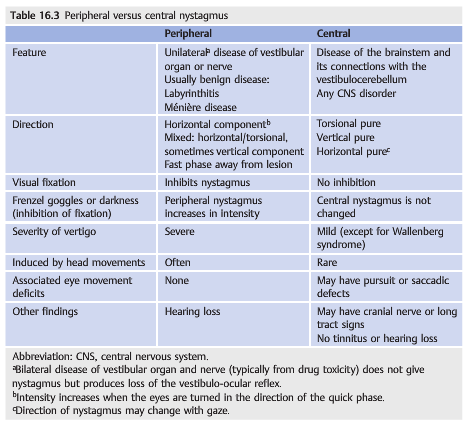
The goals of the evaluation are to decide whether there is a central or peripheral pattern of nystagmus and to determine if localization is possible based on the findings (▶Table 16.3 and ▶Table 16.4). Symptoms include oscillopsia (absent in congenital nystagmus), decreased acuity, nausea or vomiting, and vertigo.

There may be coexisting neurologic deficits.
The examination (in primary position as well as all positions of gaze) differentiates jerk from pendular nystagmus. If the finding is jerk nystagmus, look for the direction of the fast phase—watch for a few minutes, as nystagmus may occasionally alternate directions. Look for coexisting head oscillations or head turns, the effect of convergence on nystagmus, the presence of a null point (eye position where nystagmus is least prominent), and subtle nystagmus or vestibular nystagmus that is suppressed by fixation. The last can be assessed by performing ophthalmoscopy in one eye while the patient fixates at distance, then covering the fixating eye. Nystagmus may then be viewed through the ophthalmoscope (the fast phase direction is the opposite of what it appears through the direct ophthalmoscope). Frenzel goggles may be used to assess nystagmus in the absence of fixation. Electronystagmography (ENG) is another method of identifying nystagmus not present with eyes open. Finally, the Dix–Hallpike or Bárány maneuver can be done to look for positional nystagmus in patients who complain of positional vertigo (see ▶Table 16.4; ▶Fig. 16.3).

Nystagmus with Positional Vertigo
Paroxysmal vertigo occurs only in certain positions. When the Dix–Hallpike maneuver (see ▶Fig. 16.3) is performed, nystagmus is seen (see ▶Table 16.4).

Most patients have benign paroxysmal positional vertigo (BPPV) from a peripheral lesion, usually canalolithiasis or cupulolithiasis in the posterior semicircular canal. BPPV does not respond well to medications but may have a long-term favorable response to numerous maneuvers aimed at dislodging the debris from the posterior semicircular canal. Positional vertigo may also occur with central nervous system disease.
Acquired Central Nystagmus
The most important goal of the evaluation is to identify those patterns of nystagmus that have a localizing value.
Downbeat Nystagmus
Downbeat nystagmus is a type of jerk nystagmus, with the fast phase downward in the primary position (▶Fig. 16.6).

The nystagmus decreases in upgaze and worsens in downgaze; it is usually most prominent in lateral gaze and downgaze. Oscillopsia is usually prominent because the nystagmus is present in primary position and in down-gaze, the preferred reading position.
Downbeat nystagmus is caused by lesions at the cervicomedullary junction, foramen magnum, vestibulocerebellum, and medulla. It is commonly seen in cerebellar degenerations; paraneoplastic syndromes; Chiari malformation (▶Fig. 16.7); encephalitis; trauma; hypomagnesemia; thiamine deficiency; B12 deficiency; and toxicity with lithium, alcohol, amiodarone, toluene, phenytoin, and carbamazepine.

The treatment of downbeat nystagmus is limited. Removal of a toxic drug and treatment of vitamin deficiency may result in improvement. Aminopyridines, clonazepam, valproate, baclofen, and gabapentin may dampen downbeat nystagmus. Patients should be advised to avoid looking down and to not use glasses with bifocal or progressive lenses. Base-down prisms in reading glasses can be used to force the eyes upward.
Upbeat Nystagmus
Upbeat nystagmus is a type of jerk nystagmus with fast phase upward in primary position (▶Fig. 16.8). It often worsens in upgaze.

It may be caused by lesions of the medulla, cerebellar vermis, and midbrain and is commonly seen in Wernicke encephalopathy and encephalitis.
Aminopyridines and baclofen may dampen upbeat nystagmus. Patients should avoid looking up and should not use glasses with progressive lenses. Base-up prisms in reading glasses can be used to force the eyes downward.
Periodic Alternating Nystagmus
Periodic alternating nystagmus (PAN) is a type of horizontal jerk nystagmus that alternates direction in primary position (i.e., jerk nystagmus to the right for about 60 to 90seconds, which diminishes, only to begin beating to the left for another 60 to 90seconds) (▶Fig. 16.9). Patients may have a periodic alternating head turn to minimize the nystagmus, and oscillopsia is usually present.

PAN is caused by lesions of the cerebellum, particularly the nodulus and uvula, and by lesions of the cervicomedullary junction. It is commonly seen in multiple sclerosis, cerebellar degenerations (▶Fig. 16.10), Chiari malformations, trauma, hepatic encephalopathy, and albinism, as well as with use of anticonvulsants and lithium. It is responsive to baclofen.

Rebound Nystagmus
Rebound nystagmus is seen in some patients with gaze-evoked nystagmus. It is the reversal of jerk nystagmus direction after sustained eccentric gaze. Rebound nystagmus is caused by cerebellar disorders and lesions of the medulla (in the region of the nucleus prepositus hypoglossi and medial vestibular nucleus).
Brun Nystagmus
Brun nystagmus is a combination of unilateral peripheral vestibular nystagmus from an eighth nerve tumor (▶Fig. 16.11) and gaze-paretic central nystagmus as the tumor compresses the pons. It is characterized by high-frequency, low-amplitude nystagmus on looking away from the lesion, beating in the direction of gaze (due to the vestibular lesion), and low-frequency, high-amplitude horizontal nystagmus on looking toward the lesion, beating in the direction of gaze (due to defective gaze holding). Brun nystagmus is caused by large tumors in the cerebellopontine angle.
Dissociated Jerk Nystagmus
Dissociated jerk nystagmus refers to nystagmus that is different in the two eyes. The most common cause is internuclear ophthalmoplegia (adduction deficit associated with contralateral abducting nystagmus) (▶Fig. 16.12). The abducting nystagmus may be an adaptive mechanism to overcome the adduction paresis.

Acquired Pendular Nystagmus
One of the most common types of nystagmus is acquired pendular nystagmus, which is visually disabling because of severe oscillopsia (▶Fig. 16.2).It most commonly is caused by multiple sclerosis. Oscillopsia may improve with gabapentin, memantine, clonazepam, or valproate.

Seesaw Nystagmus
Seesaw nystagmus (▶Fig. 16.13) is defined as pendular nystagmus with elevation and intorsion of one eye simultaneous with depression and extorsion of the other eye, followed by a reversal of the cycle, so that the eyes move like a seesaw.

Seesaw nystagmus produces very disabling oscillopsia that responds poorly to any treatment. It is most often caused by parasellar lesions and may be seen with pituitary tumors (▶Fig. 16.14), craniopharyngiomas, septo-optic dysplasia, and brainstem lesions (especially in the midbrain).

Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.