Questions:
25. What is oculopalatal myoclonus?
26. What is oculomasticatory myorhythmia?
27. What is convergence retraction nystagmus?
28. What is superior oblique myokymia?
29. What is ocular bobbing?
30. What are saccadic intrusions?
31. What is ocular flutter?
32. What is opsoclonus?
33. What are the causes of ocular flutter and opsoclonus?
34. What is ocular dysmetria?
35. What is voluntary nystagmus?
36. What disease must be considered when a patient has confusion, ataxia, ophthalmoplegia (any pattern) and nystagmus?
____________________________________________________
Questions with answers:
25. What is oculopalatal myoclonus?
Oculopalatal myoclonus is a type of vertical pendular nystagmus coexisting with a tremor of the palate and/or facial muscles, larynx, and diaphragm. It is present during sleep. It usually develops months after an infarction or hemorrhage involving the Mollaret triangle (the region connecting the red nucleus to the inferior olive and the dentate nucleus); but can also be delayed after trauma to this region. The condition may improve with gabapentin, anticholinergic agents, or ceruletide.
Video: http://morancore.utah.edu/section-05-neuro-ophthalmology/oculopalatal-myoclonus-after-stroke/
26. What is oculomasticatory myorhythmia?
Oculomasticatory myorhythmia is defined as pendular nystagmus with pendular convergence and divergence movements of the eyes, with occasional movements of the jaw, face, or limbs. Concurrent synchronous contraction of masticatory muscles (e.g. masseter, genioglossus) but not palatal muscle characterizes this condition. It is often associated with a supranuclear vertical gaze palsy and is pathognomonic of Whipple disease.
Video: https://collections.lib.utah.edu/details?id=188601
27. What is convergence retraction nystagmus?
Convergence-retraction nystagmus is not truly nystagmus, but rather bilateral adducting saccades causing convergence of both eyes, without any slow phase. It is most often elicited by having the patient attempt to look up, at which time the eyes converge and retract in the orbit. The retraction is best seen by observing the patient from the side. Co-contraction of the horizontal rectus causes the retraction. Convergence-retraction nystagmus is one of many signs of the Parinaud dorsal midbrain syndrome (upgaze paresis, light-near dissociation of the pupils, and upper eyelid retraction). It is caused by midbrain/posterior commissure lesions.
Video: https://collections.lib.utah.edu/details?id=180330
28. What is superior oblique myokymia?
Superior oblique myokymia is defined as an oscillation of one eye due to the intermittent firing of the superior oblique muscle (myokymia or tremor of the superior oblique muscle). It produces oscillopsia or intermittent diplopia and is characterized by monocular, rapid, torsional movements. It is more easily seen at the slit lamp or with an ophthalmoscope. Superior oblique myokymia is usually benign, and no underlying etiology is found. However, neuroimaging is recommended, looking for posterior fossa tumors. Superior Oblique myokymia is usually chronic with periods of remission.
Videos: 1. http://morancore.utah.edu/section-05-neuro-ophthalmology/superior-oblique-myokymia/
2. http://morancore.utah.edu/section-05-neuro-ophthalmology/superior-oblique-myokymia-video-2/
29. What is ocular bobbing?
Ocular bobbing is characterized by conjugate eye movements beginning with a fast downward movement, followed by a slow drift back to the midline (similar to a fish bob in the water). It is commonly found in comatose patients with a massive pontine lesion or metabolic encephalopathy.
Video: https://collections.lib.utah.edu/details?id=188465
30. What are saccadic intrusions?
“Saccadic intrusions are irregular episodic occurrences of a series of two or more fast eye movements. They are classified according to whether or not the intrusive saccades are separated by a brief interval in which the eyes are stationary. Among the intrusions that lack an intersaccadic interval (‘back-to-back saccades’) are opsoclonus, ocular flutter, and so-called voluntary nystagmus. Among those with such an interval are square wave jerks, macro square wave jerks, and macro-saccadic oscillations.”2
Saccadic intrusions are often mistaken for nystagmus. In contrast to nystagmus, in which there is always a slow-phase eye movement, saccadic oscillations are saccades (rapid refixational eye movements) without any slow phases.
Video: https://collections.lib.utah.edu/details?id=1209728
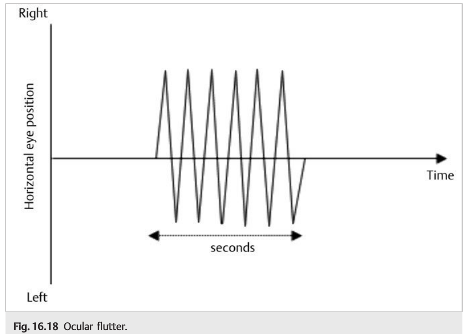
31. What is ocular flutter?
Ocular flutter is characterized by intermittent bursts of back-to-back horizontal saccades without any interval between saccades. There is no vertical component. Bursts of ocular flutter typically last for seconds at a time. The strictly horizontal direction distinguishes ocular flutter from opsoclonus, and the lack of interval between the saccades distinguishes ocular flutter from square-wave jerks.
Video: http://morancore.utah.edu/section-05-neuro-ophthalmology/ocular-flutter/
32. What is opsoclonus?
In opsoclonus there are back-to-back saccades in multiple directions, including horizontal, vertical, and torsional (sometimes referred to as saccadomania). These movements are higher amplitude and last longer than typical ocular flutter. These eye movements are often associated with blinking, facial twitching, myoclonus, and ataxia (“dancing eyes and dancing feet”).
Videos: 1. Neonatal https://collections.lib.utah.edu/details?id=188615&q=opsoclonus
2. Parainfectious https://collections.lib.utah.edu/details?id=188616&q=opsoclonus
33. What are the causes of ocular flutter and opsoclonus?
1. Paraneoplastic: Neuroblastoma in children: 50% of children with opsoclonus harbor neuroblastoma; 2% of children with neuroblastoma have opsoclonus. Small cell carcinomas and other cancers associated with anti-Ri antibodies in adults.
2. Encephalitis, cerebellitis
3. Intracranial tumor
4. Hydrocephalus
5. Thalamic hemorrhage
6. Multiple sclerosis
7. Nonketotic hyperosmolar coma
8. Drug toxicity (lithium, phenytoin, and cocaine)
34. What is ocular dysmetria?
In ocular dysmetria, the eye overshoots (saccadic hypermetria) or undershoots (saccadic hypometria) the target upon refixation. It then saccades back or forward to the intended fixation point (back-up or catch-up saccade). It is a sign of cerebellar dysfunction similar to limb dysmetria.
Video: https://collections.lib.utah.edu/details?id=188452
35. What is voluntary nystagmus?
Some normal subjects can induce ocular oscillations (often with convergence and subtle movements of the eyelids such as squinting) mimicking ocular flutter accompanied by convergence effort.
Video: https://collections.lib.utah.edu/details?id=188469
36. What disease must be considered when a patient has confusion, ataxia, ophthalmoplegia (any pattern) and nystagmus?
Wernicke encephalopathy (vitamin B1 deficiency—occurs most often in the setting of alcoholism and bariatric surgery) may produce any type of nystagmus. Intravenous thiamine should be given to any confused patient with nystagmus. Brain MRI often shows symmetric increased T2 signal intensity in the mammillary bodies, the medial thalami, the tectal plate, and the periaqueductal area. Treatment with vitamin B1, hydration, and appropriate nutrition is urgent to prevent irreversible dementia.
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme.1
Oculopalatal Myoclonus (or Tremor)
Oculopalatal myoclonus is a type of vertical pendular nystagmus coexisting with tremor of the palate and/or facial muscles, larynx, and diaphragm. It is present during sleep. It usually develops months after an infarction or hemorrhage involving the Mollaret triangle (the region connecting the red nucleus to the inferior olive and the dentate nucleus; ▶Fig. 16.15) but can also be delayed after trauma to this region. The condition may improve with gabapentin, anticholinergic agents, or ceruletide.

Oculomasticatory Myorhythmia
Oculomasticatory myorhythmia is defined as pendular nystagmus with pendular convergence and divergence movements of the eyes, with occasional movements of the jaw, face, or limbs. It is often associated with a supranuclear vertical gaze palsy and is pathognomonic of Whipple disease.
Pearls
Wernicke encephalopathy (vitamin B1 deficiency-occurs most often in the setting of alcoholism and bariatric surgery) may produce any type of nystagmus. Intravenous thiamine should be given to any confused patient with nystagmus.
16.1.4 Management of Nystagmus
The aim of management is to improve oscillopsia and/or visual blurring. Drug therapy is often empirical; there are usually poor results, except for PAN and some cases of acquired pendular nystagmus. Commonly used medications include the following:
● Baclofen (periodic alternating nystagmus)
● Gabapentin (acquired pendular nystagmus)
● Memantine (acquired pendular nystagmus)
● Aminopyridines (downbeat and upbeat nystagmus)
● Clonazepam
● Valproate
● Trihexyphenidyl or other anticholinergics
Other treatment possibilities are prisms to move the null point into primary position or away from a triggering gaze (i.e., move the eyes up in cases of downbeat nystagmus), or to induce convergence; contact lenses to dampen the nystagmus; eye muscle surgery (Kestenbaum procedure) to move the null point into primary position; and injection of botulinum toxin in the extraocular muscles to immobilize the eye (but this induces diplopia and often requires patching of one eye).
16.2 Other Nystagmoid Eye Movements
16.2.1 Convergence–Retraction Nystagmus
Convergence–retraction nystagmus (▶Fig. 16.16a) is not truly nystagmus, but rather bilateral adducting saccades causing convergence of both eyes, without any slow phase. It is most often elicited by having the patient attempt to look up, at which time the eyes converge and retract in the orbit. The retraction is best seen by observing the patient from the side. Convergence–retraction nystagmus is one of many signs of Parinaud dorsal midbrain syndrome (upgaze paresis, light-near dissociation of the pupils, and upper eyelid retraction). It is caused by midbrain/posterior commissure lesions (▶Fig. 16.16b).

16.2.2 Superior Oblique Myokymia
Superior oblique myokymia (▶Fig. 16.17) is defined as oscillation of one eye due to intermittent firing of the superior oblique muscle (myokymia or tremor of the superior oblique muscle).

It produces oscillopsia or intermittent diplopia, elicited by having the patient look in the direction of the superior oblique muscle, and is characterized by monocular, rapid, intorsional movements. It is best seen at the slit lamp or with an ophthalmoscope. Superior oblique myokymia is usually benign, and no underlying etiology is found. However, neuroimaging is recommended, looking for posterior fossa tumors. Superior oblique myokymia is usually chronic with periods of remission.
Treatment includes carbamazepine, baclofen, or propranolol. Surgical weakening of the superior oblique muscle may be performed in refractory cases.
16.2.3 Ocular Bobbing
Ocular bobbing is characterized by conjugate eye movements beginning with a fast downward movement, followed by a slow drift back to the midline (similar to a fish bob in the water). It is commonly found in comatose patients with a massive pontine lesion or metabolic encephalopathy.
16.3 Saccadic Intrusions
Saccadic intrusions are often mistaken for nystagmus. In contrast to nystagmus, in which there is always a slow-phase eye movement, saccadic oscillations are saccades (rapid refixational eye movements) without any slow phases.
16.3.1 Ocular Flutter
Ocular flutter (▶Fig. 16.18) is characterized by intermittent bursts of back-to-back horizontal saccades without any interval between saccades. There is no vertical component. Bursts of ocular flutter typically last for seconds at a time. The strictly horizontal direction distinguishes ocular flutter from opsoclonus, and the lack of interval between the saccades distinguishes ocular flutter from square-wave jerks.
16.3.2 Opsoclonus
Opsoclonus is back-to-back saccades in multiple directions, including horizontal, vertical, and torsional (sometimes referred to as saccadomania). These movements are higher amplitude and last longer than typical ocular flutter. Eye movements are often associated with blinking, facial twitching, myoclonus, and ataxia (“dancing eyes and dancing feet”).
Causes of Ocular Flutter and Opsoclonu
Causes of ocular flutter and opsoclonus include the following:
● Paraneoplastic:
○ Neuroblastoma in children: 50% of children with opsoclonus harbor a neuroblastoma; 2% of children with neuroblastoma have opsoclonus.
○ Small cell carcinomas and other cancers associated with anti-Ri antibodies in adults
● Encephalitis, cerebellitis
● Intracranial tumor, hydrocephalus, thalamic hemorrhage, multiple sclerosis, nonketotic hyperosmolar coma, drug toxicity (lithium, phenytoin, and cocaine)
16.3.3 Square-Wave Jerks and Macrosquare-Wave Jerks
Horizontal to-and-fro saccades that interrupt fixation are referred to as square wave jerks (▶Fig. 16.19). Unlike ocular flutter, square-wave jerks have intersaccadic intervals. They are termed macrosquare-wave jerks when the amplitude is>5 degrees. Common causes include cerebellar diseases, Parkinson disease, and progressive supranuclear palsy.

16.3.4 Ocular Dysmetria
In ocular dysmetria, the eye overshoots (saccadic hypermetria) or undershoots (saccadic hypometria) the target upon refixation. It then saccades back or forward to the intended fixation point (back-up or catch-up saccade). It is a sign of cerebellar dysfunction similar to limb dysmetria.
16.3.5 Voluntary Nystagmus
Some normal subjects can induce ocular oscillations (often with convergence and subtle movements of the eyelids such as squinting) mimicking ocular flutter accompanied by convergence effort.
16.4 Summary of the Evaluation of the Patient with Ocular Oscillations (▶Fig. 16.20)
The diagram below summarizes the steps necessary for the characterization of ocular oscillations.

References: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
2. Canadian Neuro-Ophthalmology Group Textbook-XI. Saccadic Intrusions
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.